

Imagine working a 24/7 job with zero vacation days, where a single math error at lunch could land you in the emergency room. That is the relentless reality of tracking carbs, calculating insulin, and dodging judgmental stares in our society.
Protecting your mental health with type 1 diabetes in india is just as critical as monitoring your HbA1c, yet this emotional weight is rarely discussed in regular clinic visits. When chronic exhaustion turns into total emotional paralysis, you aren’t weak—you are experiencing a medically recognized state called diabetes burnout.
If you are drowning under endless finger-pricks, high out-of-pocket costs, or agonizing marriage market stigma, your exhaustion is real. Let’s break down the science of this psychological fatigue and how to reclaim your life.
What Is Diabetes Burnout — And Why It Is More Common in India Than You Think
Diabetes burnout is total physical and mental exhaustion from the relentless, 24/7 demands of managing this chronic condition. Imagine counting every carb in your meal, tracking blood sugar, and injecting insulin every single day without a single day off. Eventually, the mind feels paralyzed by this constant vigilance. This leads to a dangerous coping mechanism known as a “diabetes vacation”—where a patient intentionally skips insulin doses, ignores dietary restrictions, or stops finger-pricks just to feel “normal” for a moment.
While burnout is a universal struggle, it hits much harder in India due to deep-rooted cultural and systemic pressures:
- The Burden of “Being Othered”: Despite housing nearly 90 million adults with diabetes and the world’s highest number of Type 1 Diabetes (T1D) cases, Indian society is often unsupportive. Patients face discrimination and are wrongly treated as “sick” or “dependent.”
- A “Prick-Sensitive” Culture: Publicly injecting insulin or managing glucose monitor alarms triggers intense social judgment and unwanted stares, forcing many into isolation.
- The Marriage Market Nightmare: Unfounded myths surrounding fertility and lifespan make finding a spouse a massive source of anxiety. Families often resort to agonizing secrecy to avoid social rejection, heavily impacting young women.
- Financial and Psychological Gaps: High out-of-pocket expenses for medical supplies, paired with a severe shortage of diabetes psychologists, leave families completely stranded.
Tragically, up to 20% of Indian children with T1D suffer from ignored psychosocial struggles, driving a downward spiral of poor glycemic control and frequent hospitalizations.
Signs You or Your Child May Be Experiencing Diabetes Burnout Right Now
Diabetes burnout manifests differently depending on who is carrying the load. Recognizing these signs early is critical to preventing severe clinical complications like Diabetic Ketoacidosis (DKA) or deep psychological distress.
1. In Adults: The Silent Withdrawal
- The “Diabetes Vacation”: Intentionally unplugging CGMs, skipping finger-pricks, or guessing insulin doses just to escape the disease.
- Decision Paralysis: Chronic mental fatigue from making hundreds of blood-sugar choices a day, leading to total apathy toward self-care.
- Social & Eating Shifts: Avoiding social gatherings to escape public judgment, or developing disordered eating—such as diabulimia (the highly dangerous practice of omitting insulin for weight loss).
2. In Children & Teens: The Outward Rebellion
- Active Non-Adherence: Refusing insulin injections, sneaking food, or falsifying blood sugar logbooks.
- Behavioral Shifts: Sudden aggression, slipping school grades, and explosive arguments with parents over diabetes management.
3. In Parents: Caregiver Chronic Fatigue
- Alarm Fatigue & “Brain Fog”: Severe sleep deprivation from checking nighttime blood sugars, causing profound daytime memory and concentration issues.
- The Guilt Loop: Feeling intense, ongoing grief over their child’s condition, often paired with guilt for neglecting healthy siblings due to intensive diabetes management demands.
Clinical Insight: These behaviors are not signs of defiance or laziness. They are a physiological and emotional cry for help. If you recognize these symptoms, the solution is not stricter rules—it is psychological support and diabetes distress management.
Depression & Anxiety in Type 1 Diabetes: How Common Is It Among Indians?
Living with Type 1 Diabetes (T1D) is as much a mental health battle as it is a metabolic one. Globally, nearly 1 in 3 people with T1D battle clinically significant depression (30.4%) and anxiety (32%). In India, this crisis hits early, affecting 20% of children living with the condition.
For South Asians, the risk of developing depression alongside diabetes escalates with age, financial strain, or a family history of psychiatric illness. However, the most profound, unique trigger in India is marital stigma.
Due to baseless societal myths regarding fertility and lifespan, young T1D patients—particularly women—face immense discrimination in the marriage market. The agonizing fear of rejection, social isolation, and higher divorce rates inflict deep psychological trauma.
The clinical consequences of ignoring this distress are dangerously cyclical:
Mental Stress (Anxiety/Depression)
│
Spike in Stress Hormones (Cortisol/Adrenaline)
│
Erratic Blood Sugars & Poor Metabolic Control
│
Higher Hospitalizations & Long-Term Complications
Despite these severe risks, psychosocial care is frequently ignored in routine Indian clinical practice.
Mental health is not secondary to diabetes care—it is diabetes care. Emotional distress physically alters your blood biochemistry, making optimal glycemic control nearly impossible without psychological support.
The Emotional Burden on Parents of Children with Type 1 Diabetes in India
When a child is diagnosed with Type 1 Diabetes (T1D), parents don’t just absorb medical data; they mourn the loss of a “normal” childhood. This initial shock quickly hardens into a state of permanent hyper-vigilance.
- The Nighttime Vigil: The terrifying fear of nocturnal hypoglycemia (dangerous nighttime low blood sugar) causes chronic sleep deprivation. Parents become prisoners to continuous glucose monitor (CGM) alarms, leading to severe daytime brain fog.
- The Culture of Secrecy: In India’s “prick-sensitive” society, rampant misconceptions force families into painful isolation. Fearing social stigma, parents often hide the diagnosis from relatives, cutting off their own emotional safety nets.
- The Matrimonial Anxiety: Unfounded myths claiming T1D causes infertility or structural disability turn future marriage prospects—especially for daughters—into a source of deep parental despair.
- Spousal Strain & Sibling Guilt: The relentless pressure frequently fractures marriages, sometimes triggering misplaced blame for the condition. It also fuels “sibling guilt,” as healthy children are forced to grow up prematurely while diabetes consumes the family’s time and finances.
- The School & Financial Void: With zero universal healthcare funding and a distinct lack of diabetes training in Indian schools, parents carry the entire physical and financial burden entirely alone.
Clinical Reality: Caregiver burnout directly impacts patient outcomes. A stressed, sleep-deprived parent is more prone to insulin dosing errors. Supporting the parent’s mental health is biochemically essential for managing the child’s blood sugars.
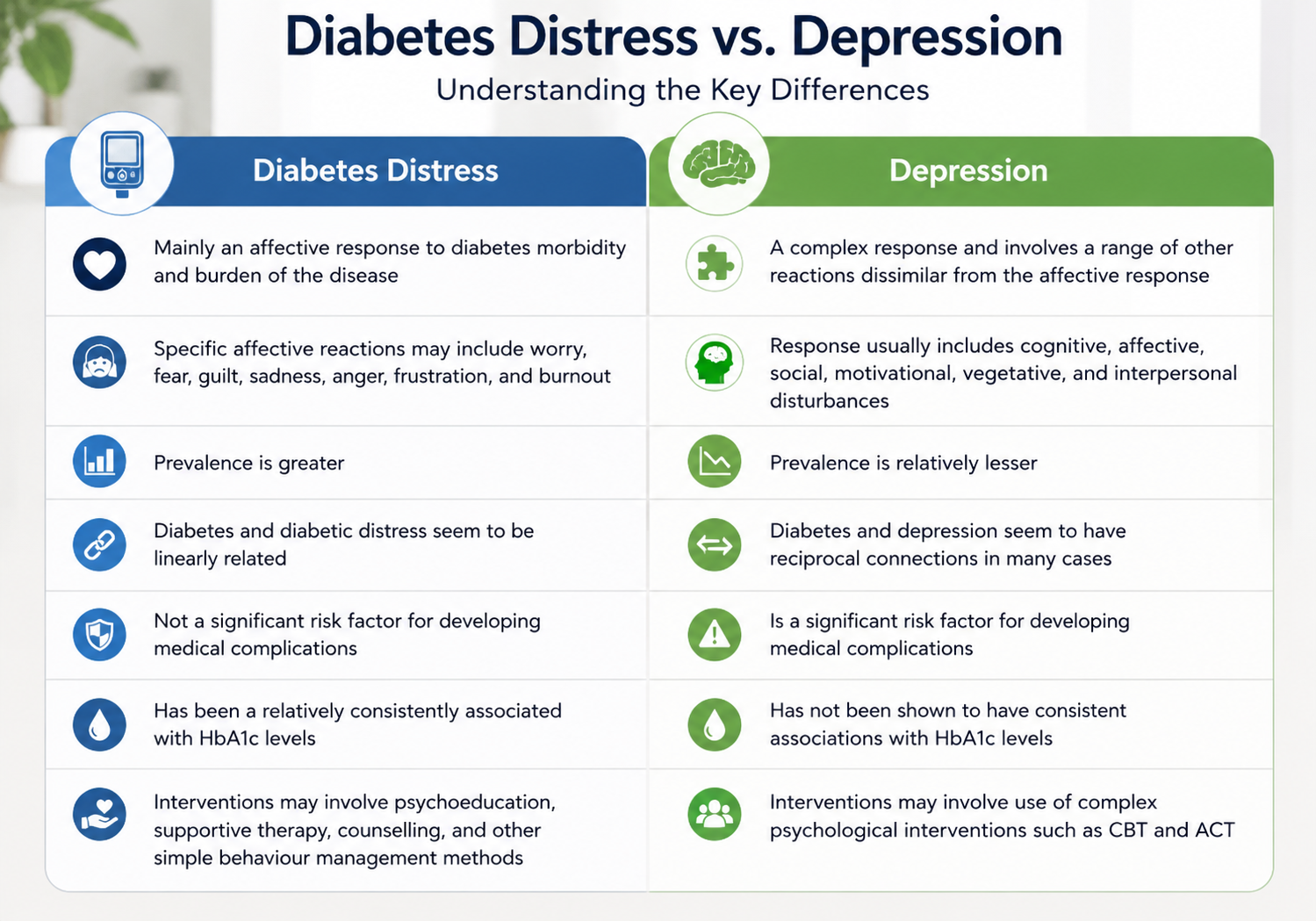
Diabetes Distress vs Clinical Depression: Understanding the Difference
It is easy to confuse feeling overwhelmed by your health with a psychiatric condition. However, a critical medical distinction exists between Diabetes Distress and Clinical Depression.
- Diabetes Distress: A natural emotional reaction to the unrelenting, 24/7 mental load of managing diabetes. It is explicitly tied to your condition—the daily exhaustion of blood sugar spikes, insulin calculations, and finger-pricks.
- Clinical Depression: A broader mental health condition that dampens your mood across all aspects of life. It is characterized by pervasive sadness, feelings of worthlessness, and anhedonia (the total inability to experience joy), independent of your diabetes.
Because physical fatigue and sleep disruptions overlap, routine clinical surveys frequently yield “false positives,” misdiagnosing standard diabetes burnout as major depressive disorder.
However, they can dangerously interact. Severe caregiving or management distress can trigger underlying depressive episodes. Conversely, clinical depression introduces avolition (a severe lack of motivation). Because Type 1 Diabetes forces patients to physically mobilize to take insulin and stay alive, family members often wrongly minimize their suffering, completely missing a patient’s deep depression because they are still managed to perform daily survival tasks.
Accurate diagnosis requires looking at the root. If your psychological exhaustion is entirely bound to blood sugars and device failures, it is diabetes distress—which requires supportive care and lifestyle adjustments, not traditional psychiatric medication.
How Indian Families Can Support a Loved One Living with Type 1 Diabetes
Type 1 Diabetes is never a solo diagnosis—it is a family condition. In India, a supportive home environment is the single most powerful buffer against both diabetes burnout and corrosive societal stigma.
- Share the Caregiving Load: The 24/7 mental load often breaks the primary caregiver (usually the mother). Extended family members must learn to check blood glucose and administer insulin, providing vital backup to prevent caregiver burnout.
- Avoid Premature Autonomy: Clinical guidelines warn that forcing children or teens to handle their diabetes care completely alone too early spikes diabetes distress, directly driving up HbA1C levels. Balance protective care with gradual independence.
- Dismantle the Blame Game: Because T1D is an autoimmune condition, families must eliminate toxic, unscientific blame (pointing fingers at a spouse’s lineage, diet, or past vaccines). Fostering an open, judgment-free environment helps patients share their management struggles safely.
- Fiercely Combat Marital Stigma: Protect your loved one against “prick-sensitive” social judgment. Bring prospective spouses to your diabetes care team for direct medical education to debunk groundless myths about fertility and genetics.
- Protect Siblings & Allow Breaks: Ensure healthy siblings aren’t emotionally sidelined. Additionally, support your loved one if they need a medically supervised “data vacation”—briefly stepping back from hyper-analyzing constant CGM alerts to prevent mental paralysis.
A supportive, educated home environment directly correlates with lower glucose variability and enhanced illness adaptation. Family involvement isn’t just an emotional luxury; it actively improves medical outcomes.
Navigating Social Stigma & Marriage Pressure with Type 1 Diabetes in India
In India, a Type 1 Diabetes (T1D) diagnosis doesn’t just alter your biochemistry—it alters your social standing. Our “prick-sensitive” society often treats public insulin shots or beeping CGMs with judgmental stares, forcing young adults into painful secrecy and isolation.
This psychological weight peaks in the arranged marriage market, hitting young women hardest. Families face agonizing anxiety due to cruel, unscientific myths claiming T1D means infertility or a severely shortened lifespan.
Another massive roadblock is the genetics myth. Let’s clear the air with hard medical data: over 85% of people with T1D have no family history of it. If a mother has T1D, the risk of passing it to her child is only about 2%. If the father has it, it is just 4.6%. Fear of disclosing daily realities—like nighttime lows or hypoglycemia during intimacy—causes many to avoid relationships entirely.
How to Dismantle the Stigma
- Pre-Marital Care-Team Education: Bring your prospective partner to your endocrinologist. Real clinical facts dismantle fear, proving that normal, healthy pregnancies are entirely achievable.
- Spousal Collaboration: When a partner actively shares the management load, patient blood sugar control drastically improves.
- Peer Communities: Join local T1D support groups to rebuild self-esteem and learn to live loudly with your tech.
Mindfulness, Yoga & Stress Management Specifically for Type 1 Diabetes
When you are stressed, your body releases hormones like cortisol and adrenaline. Biochemically, these stress hormones act like a roadblock, forcing your liver to dump extra glucose into your bloodstream while making your body resistant to insulin. Therefore, stress management isn’t a luxury—it is a clinical necessity for optimal glycemic control.
To lower your HbA1C and defeat burnout, integrate these evidence-based psychological tools:

- Mindful Self-Compassion: Studies prove that practicing daily mindful breathing lowers depression and reduces diabetes distress, directly improving A1C levels. Under medical guidance, this can include a structured “data pause”—temporarily stepping back from overwhelming CGM alarms for a mental reset.
- Yoga (2–3 times/week): Yoga actively downregulates your sympathetic nervous system (the “fight-or-flight” response). Combined with standard aerobic exercise, it provides vital mental relaxation and vascular benefits.
- Behavioral Therapies (CBT & ACT): Cognitive Behavioral Therapy (CBT) and Acceptance and Commitment Therapy (ACT) build “psychological flexibility.” This cognitive conditioning helps patients and parents reframe negative self-talk, protecting against caregiver burnout.
- Peer Support Groups: Connecting with fellow T1D communities is clinically shown to boost medication adherence, reduce isolation, and improve overall quality of life.
Managing your mind directly changes your blood chemistry. True Type 1 Diabetes care requires balancing your daily insulin units with psychological resilience.
Where to Get Mental Health Support for Diabetes in India: Helplines & Communities
You do not have to carry the relentless, 24/7 mental load of diabetes entirely on your own. When burnout paralyzes your self-care, think of mental health resources as your clinical “pit crew.” India has specialized, free, and institutional support systems designed to help you and your family recalibrate.
Immediate & Professional Support
- Tele MANAS Helpline: For free, round-the-clock confidential mental health counseling, dial 14416 or 1800-891-4416. This National Tele Mental Health Programme connects you instantly to trained professionals.
- NIMHANS (Bangalore): India’s premier mental health institute offers dedicated care for chronic illness distress through the Sakalwara Community Centre (offering vital telemedicine) and the NIMHANS Centre for Well Being.
Community & Peer Support Networks
- The Diabetes Online Community (DOC): Finding your “tribe” through digital peer support networks provides shared humor, practical coping strategies, and directly dismantles the societal “burden of being othered.”
- Shared Medical Appointments (SMAs) & Diabetes Camps: Many Indian centers organize group clinic sessions and camps. Combining peer-to-peer problem-solving with direct access to your medical team is clinically proven to stabilize glycemic control and improve overall quality of life.
How to Activate Your Care Team: Modern clinical guidelines explicitly mandate that behavioral health is an integral part of diabetes management. At your next check-up, ask your endocrinologist directly: “Do you have a specialized clinical psychologist or medical social worker integrated into your team who understands diabetes distress?”
Online Diabetes Communities in India: Facebook Groups, WhatsApp & Forums
When you are managing Type 1 Diabetes (T1D), isolation can feel heavier than the clinical disease itself. This is where the Diabetes Online Community (DOC) becomes an essential part of your management plan. Connecting with peers who share your exact daily struggles lowers diabetes distress, replaces fear with shared humor, and actively improves your long-term metabolic control.
In India’s “prick-sensitive” culture, finding your digital tribe is the fastest way to shatter social stigma and forced secrecy. Instead of hiding your medical devices, you can plug into massive, active, patient-led Indian networks:
- Blue Circle Diabetes Foundation: India’s largest patient-led NGO. They run a thriving Facebook community called Diabetes Support Network – India, localized regional WhatsApp groups, and a free, custom mobile app featuring anonymous peer forums and a “Buddy Project” helpline.
- Type 1 Diabetes Foundation of India (T1DF): A dedicated non-profit focusing on T1D education, policy advocacy, and community-driven regional support networks across Indian cities.
Clinical literature proves that peer-led intervention dramatically boosts medical adherence and emotional resilience. You do not have to calculate insulin doses or manage sensor alarms in the dark. Join these groups to stop feeling isolated and start thriving.
When to See a Mental Health Professional: A Clear Guide for T1D Patients & Families
While managing Type 1 Diabetes (T1D) involves an expected emotional toll, clinical guidelines emphasize that certain milestones and behaviors require specialized behavioral health support. Seeking therapy is not a failure; it is a vital clinical intervention to protect both your metabolic and mental health.
Immediate Clinical “Red Flags”
Consult a mental health specialist immediately if you notice:
- Self-Care Abandonment: Completely stopping blood checks, ignoring dietary restrictions, or experiencing total decision paralysis.
- Diabulimia: The highly dangerous practice of omitting or underdosing insulin specifically to lose weight.
- Recurrent Emergencies: Repeated hospitalizations for Diabetic Ketoacidosis (DKA) or frequent, severe low blood sugar episodes.
- Youth Exhaustion: A sudden drop in school grades, severe aggression, or a child expressing deep hopelessness and self-harm.
Chronic Burnout & Caregiver Distress
Diabetes distress requires targeted therapy when routine endocrinologist visits fail to ease your constant worry. For adults, this looks like pervasive anhedonia—the complete inability to experience joy. For parents, it manifests as severe “brain fog” from chronic sleep deprivation due to nighttime alarms, intense “sibling guilt,” or severe marital strain over the division of caregiving labor.
Navigating Indian Societal Pressures
Preemptive counseling is critical during high-stress life transitions:
- The Marriage Pressure Cooker: Navigating India’s arranged marriage market causes immense psychological trauma due to rampant myths surrounding fertility and genetics. Joint counseling for the family and the prospective spouse protects the patient’s mental health.
- Care Transitions: Shifting from pediatric to adult healthcare during late adolescence is a high-risk zone for fragmented medical care and worsening HbA1C levels.
Modern clinical frameworks mandate that behavioral health professionals are integral members of the diabetes interprofessional team. Treating psychological fatigue is biochemically essential to achieving optimal glycemic control.
FAQ
Can type 1 diabetes mess with mental health?
Yes, Type 1 diabetes significantly impacts mental health. The relentless daily demands of managing the disease frequently lead to severe diabetes burnout and distress. Additionally, individuals with T1D face much higher rates of clinical depression, anxiety disorders, and eating disorders compared to the general population.
What is the honeymoon phase of type 1 diabetes?
The honeymoon phase (partial remission) occurs weeks or months after a Type 1 diabetes diagnosis when residual beta cells temporarily produce insulin. During this time, patients require minimal or no exogenous insulin. Eventually, these cells are permanently lost, and insulin needs increase.
Can anxiety raise blood sugar?
Yes, anxiety and stress can significantly raise blood sugar levels. Psychological distress triggers the release of counterregulatory hormones, such as cortisol and catecholamines, which oppose insulin action and increase glucose production, ultimately resulting in elevated blood sugar.
Type 1 diabetes mental health support?
Mental health support for Type 1 diabetes involves integrating psychologists directly into your care team. Therapies like cognitive behavioral therapy and mindfulness effectively reduce distress. Additionally, joining peer support groups or the Diabetes Online Community provides crucial shared experiences and emotional relief.
Social effects of type 1 diabetes?
Type 1 diabetes frequently causes profound social isolation and forced secrecy due to public judgment over insulin use. Patients often face severe marital discrimination, wrongly perceived as sick or infertile. Additionally, the relentless caregiving burden heavily strains partner intimacy and sibling relationships.
Type 1 diabetes and depression?
Type 1 diabetes significantly increases the risk of clinical depression, with about 30.4% of patients experiencing clinically significant symptoms. The relentless mental load of daily management and societal stigma often trigger or worsen depressive episodes, creating a dangerous cycle of poor glycemic control and health complications.
What is type 1 diabetes distress?
Type 1 diabetes distress is the negative emotional burden resulting directly from the relentless daily demands of managing the illness. It encompasses the constant worry, frustration, and exhaustion tied specifically to strict medical routines, continuous vigilance, and the fear of long-term complications.
References
https://www.thelancet.com/journals/landia/article/PIIS2213-8587(25)00397-3/abstract
https://health.osu.edu/health/mental-health/managing-diabetes-and-mental-health
https://www.frontiersin.org/journals/endocrinology/articles/10.3389/fendo.2023.1095729/full
https://pmc.ncbi.nlm.nih.gov/articles/PMC6319281
https://pmc.ncbi.nlm.nih.gov/articles/PMC5838892
https://www.sciencedirect.com/science/article/abs/pii/S2212958823000034
https://themindclan.com/blog/free-mental-health-support-groups-india
https://pmc.ncbi.nlm.nih.gov/articles/PMC4439893
https://professional.diabetes.org/standards-of-care
https://diabetes.org/about-diabetes/type-1
About the Author
It’s me Mohammad Junaid Rain an MBBS student at GMC Nagpur, passionate about making evidence-based medical information accessible to every Indian. “medstuffs.com” is dedicated to clear, disease education for patients and caregivers.
Disclaimer: This article is for educational purposes only and does not substitute professional medical advice. Please consult your doctor for diagnosis and treatment.