
Your child has been drinking water all day. They are tired by noon. They have lost weight without trying. You assume it’s a growth spurt, summer heat, or a virus.
Then they collapse.
Type 1 diabetes in children India is diagnosed far too late — often in the emergency room, in a life-threatening condition called DKA. India now has the highest number of children under 20 living with T1D in the world: over 3 lakh young lives, according to the International Diabetes Federation 2024.
Yet most parents have never heard of the 4 Ts. Most teachers don’t know what to do when a child’s blood sugar crashes. And most families learn to manage insulin injections, school tiffins, and teenage hormones entirely on their own.
This guide changes that. Everything you need — from spotting the first symptoms to finding free insulin — is here, in one place, written for Indian families.
How Type 1 Diabetes Develops in Children: Inside the Body
Imagine your child’s body as a bustling city powered by glucose (sugar) from food. To enter cells and create energy, glucose needs a specific key called insulin, which is produced by pancreatic beta cells.
In Type 1 Diabetes (T1D), the immune system experiences a glitch—a case of “friendly fire”—where it mistakenly attacks and destroys these vital insulin factories.
The Starvation Crisis & DKA
Without insulin keys, sugar traps itself in the bloodstream, leaving cells starving. Desperate for energy, the body rapidly breaks down fat, creating an emergency fuel that leaves behind toxic, acidic waste called ketones. An excess buildup triggers Diabetic Ketoacidosis (DKA)—a life-threatening emergency signaled by vomiting, dehydration, and a distinct fruity breath odor.
The 3 Silent Stages
T1D is a progressive condition that develops over months or years:
- Stage 1 (Pre-symptomatic): The autoimmune attack begins. Blood sugar is normal, but immune markers (islet autoantibodies) are present.
- Stage 2 (Pre-symptomatic): More beta cells are destroyed. Blood sugar becomes abnormal, but the child still feels fine.
- Stage 3 (Symptomatic): Critical mass is lost. High blood sugar breaks through, causing sudden weight loss, extreme thirst, and frequent urination.
Triggers and the Puberty Spike
Children with specific genetic markers (like HLA-DR3/DR4) are vulnerable, but environmental triggers like enteroviruses often spark the condition. Later, puberty complicates management. Surging growth hormones cause natural insulin resistance, frequently forcing insulin requirements to skyrocket by 30% to 50% overnight.
At What Age Can a Child Get Type 1 Diabetes? From Toddlers to Teenagers
Type 1 Diabetes (T1D) can strike at any age, from infancy to adulthood. However, clinical data from the Registry of Youth Onset Diabetes in India reveals distinct age peaks where cases sharply rise:
- Toddlers (Ages 0–4) | 15.7% of cases: Diagnosis before 6 months is rare and usually points to a genetic variant called neonatal diabetes. Crucially, toddlers face the highest risk of Diabetic Ketoacidosis (DKA) because they cannot vocalize how they feel, leading to dangerous diagnostic delays.
- Primary Schoolers (Ages 5–9) | 30.7% of cases: A significant spike occurs as children enter early childhood, particularly between ages 5 and 7.
- Teens & Pre-Teens (Ages 10–19) | Over 53% of cases: The absolute peak occurs between 10 and 14 years. The culprit? Puberty. Surging growth hormones act like a roadblock to insulin, creating a natural resistance that unmasks the condition in vulnerable children.
The “4Ts” Lifesaving Checklist
Aligned with the Indian Union Health Ministry’s public awareness framework, parents must watch for the 4Ts, which manifest rapidly over days:
- Toilet: Heavy diapers or sudden, unusual bedwetting.
- Thirsty: Unquenchable, constant drinking.
- Tired: Severe exhaustion and sudden irritability.
- Thinner: Rapid weight loss despite eating normally.
If you observe these signs, consult a doctor for an immediate, simple finger-prick blood sugar test.
The 4 Ts: How to Spot Type 1 Diabetes in Your Child Before a Crisis Hits
Type 1 Diabetes (T1D) symptoms can escalate in just days. Memorizing the “4 Ts”—the clinical screening framework used to catch early onset—can save your child from a severe medical emergency.
- Toilet (Frequent Urination): Excess sugar spills into the urine, pulling water with it. Look for sudden bedwetting in potty-trained children, frequent midnight bathroom trips, or unusually heavy diapers in babies.
- Thirsty (Unquenchable Thirst): To compensate for the fluid lost in the toilet, the brain triggers a relentless, desperate thirst. Your child may gulp down entire glasses of water and still feel dry.
- Tired (Extreme Exhaustion): Because glucose cannot enter the cells to create energy, the body effectively runs on empty. A normally playful child will become profoundly lethargic and irritable.
- Thinner (Rapid Weight Loss): Starving for fuel, the body begins rapidly burning its own fat and muscle stores. You will notice rapid weight loss despite an increased appetite.
Preventing the DKA Crisis
Missing these signs can lead to Diabetic Ketoacidosis (DKA), a life-threatening emergency where toxic acids (ketones) flood the blood. Nearly 25% of children are only diagnosed after DKA strikes. Emergency warning signs include vomiting, rapid breathing, stomach pain, or a distinct fruity breath odor.
Your Next Step: If you spot even one “T,” do not wait. Request an immediate, simple finger-prick blood sugar test from your doctor. It takes seconds and provides life-saving clarity.
What Happens If Type 1 Diabetes Is Missed? Understanding DKA in Children
Missing the early “4Ts” can cause a child’s condition to rapidly spiral into Diabetic Ketoacidosis (DKA)—a life-threatening metabolic emergency. Shockingly, 1 in 4 children with Type 1 Diabetes in India are only diagnosed after reaching DKA, with toddlers under 5 facing the highest risk.
Without insulin keys, cells starve. The body panics and breaks down fat at an extreme pace, flooding the system with toxic, acidic waste called ketones. This triggers a dangerous chain reaction: the blood turns highly acidic (metabolic acidosis), while the kidneys desperately flush out sugar, causing severe dehydration.
The Dangerous Misdiagnosis Trap
Because early DKA heavily features vomiting and stomach pain, it is frequently misdiagnosed as a common stomach flu (gastroenteritis), appendicitis, or even pneumonia. Watch for these critical red flags:
- Kussmaul Breathing: Deep, rapid, heavy gasping as the lungs desperately try to exhale carbon dioxide to reduce blood acidity.
- Acetone Breath: A distinct fruity or nail-polish-remover smell.
- Altered Mental State: Sudden extreme drowsiness, confusion, or lethargy.
Why DKA is an ICU Emergency
DKA is the leading cause of death in children with T1D, primarily driven by cerebral edema (fatal brain swelling), which accounts for up to 90% of pediatric DKA deaths. Overcoming this requires immediate ICU admission for precision IV fluids, insulin drips, and electrolyte balancing. A simple, timely finger-prick blood test avoids this trauma entirely.
My Child Was Just Diagnosed with Type 1 Diabetes: What Do I Do First?
Hearing this diagnosis can feel like the world is stopping, but take a deep breath: with the right tools, your child will lead a full, vibrant life. Here is your immediate, expert-backed action plan:
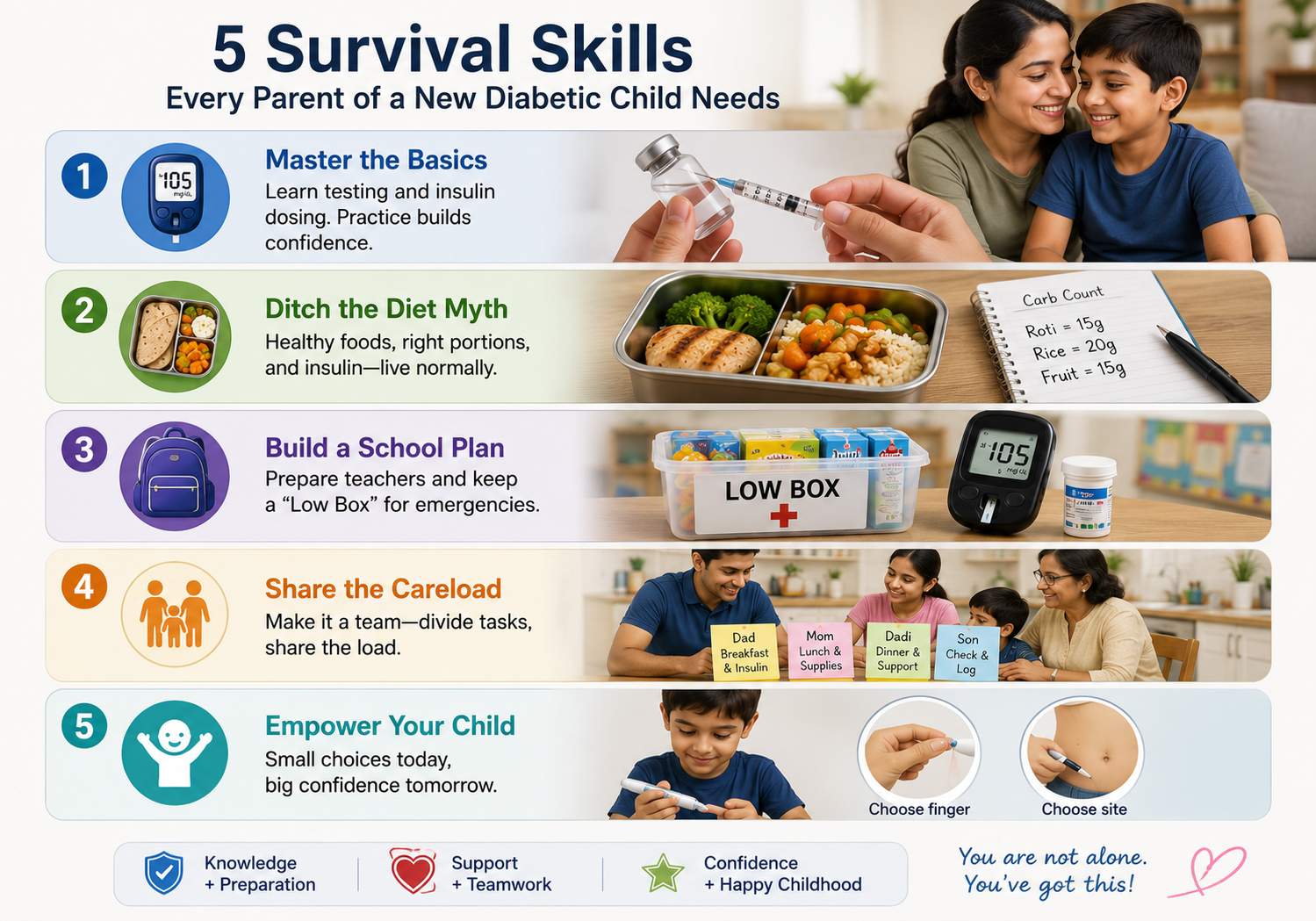
- Master the “Survival Skills”: Before leaving the hospital, your medical team will teach you blood glucose testing and insulin dosing. Pro tip: Practice giving a normal saline injection to yourself first. It conquers your fear and proves to your child that modern, micro-needles are virtually painless.
- Ditch the “Diabetic Diet” Myth: There is no restrictive food prison. Your child can eat the same healthy meals as the rest of the family. You will learn carbohydrate counting—simply matching the insulin dose to the food eaten, allowing for a flexible, normal lifestyle.
- Build a School Action Plan: Meet with teachers and principals to map out a care routine. Provide the classroom with a “Low Box” packed with fast-acting sugars (juice boxes or glucose tablets) and backup testing supplies for emergencies.
- Share the Careload: Diabetes management is a team sport. Divide daily tasks among family members so the emotional and physical burden does not crash onto one person (frequently mothers).
- Empower Your Child: Even at age 5, let them choose which finger to prick or select their injection site. Small choices give them back a sense of control over their own body.
Insulin Injections for Children: Types, Timing, Doses & Reducing Pain
Caring for a child with Type 1 Diabetes (T1D) means manually mimicking an organ.
1. Types of Insulin and Timing
Think of your child’s insulin regimen as a combination of a foundational anchor and a fire extinguisher:
- Basal (Background): Long-acting analogs (Glargine, Degludec) provide a steady, 24-hour baseline whisper of insulin to keep blood sugar stable overnight and between meals.
- Bolus (Mealtime): Rapid-acting insulins (Aspart, Lispro) act like quick fire extinguishers to neutralize sugar spikes from food. Administer these 15 to 20 minutes before meals.
- The Toddler Exception: If you have an unpredictable preschooler prone to food refusal, inject rapid insulin during or right after the meal based on what they actually swallowed to prevent dangerous low blood sugar (hypoglycemia).
2. Dosing Shifts & The Golden Sick-Day Rule
Insulin requirements are fluid. During the early “honeymoon phase,” the pancreas temporarily sputters back to life, lowering needs below 0.5 units/kg/day. Conversely, pubertal growth hormones trigger intense insulin resistance, causing teenage doses to skyrocket up to 2.0 units/kg/day.
The Medical Baseline: Infection and fever flood the body with stress hormones that drive blood sugar up—even if your child isn’t eating. Never completely stop insulin on sick days, as this rapidly triggers life-threatening Diabetic Ketoacidosis (DKA).
3. Proven Strategies to Eliminate Needle Anxiety
Modern needles are incredibly thin, but parental technique dictates the comfort level:
- Skip the Alcohol Swabs: Wet alcohol strips the needle’s pain-reducing silicone coating. Wash the skin with basic soap and water instead.
- Inject Room-Temperature Insulin: Cold insulin stings. Keep the currently active pen out of the fridge.
- Meticulous Site Rotation: Move each injection one inch away from the last spot. Repetitive punctures cause lipohypertrophy (rubbery fat lumps), which delays insulin absorption and causes wild blood sugar swings.
- Consider an Injection Port: Subcutaneous ports (like the i-Port) stay on the skin for 3 days. You inject directly into the port, reducing physical skin punctures from 12 down to just 1 every few days.
Blood Sugar Targets for Children with Type 1 Diabetes in India
Managing pediatric diabetes requires a clear roadmap. The Indian Council of Medical Research (ICMR) aligns its official frameworks with global bodies like ISPAD to give families safe, everyday blood glucose milestones.
Daily Finger-Prick & HbA1c Benchmarks
For routine daily monitoring, look for these foundational blood sugar numbers:
- Pre-meal: 70 to 130 mg/dL
- Post-meal (1-2 hours after eating): 90 to 180 mg/dL
- Bedtime: 80 to 140 mg/dL
Your golden three-month average marker, the HbA1c test, should ideally sit below 7.0%. This balances strict organ protection with a safety buffer against severe low blood sugar.
Continuous Glucose Monitors (CGM) & Time in Range
If your child utilizes a wearable Continuous Glucose Monitor (CGM) sensor, your primary clinical target shifts to a metric called Time in Range (TIR).
The goal is to keep your child’s blood sugar sitting stably within the 70–180 mg/dL “safety zone” for greater than 70% of the day.
Why Your Doctor Must Individualize Targets
Clinical averages are just baselines; an expert endocrinologist will customize targets based on development:
- Toddlers (Under 6): Targets are deliberately kept more relaxed (higher) because tiny children cannot articulate or realize when they are experiencing a “low,” which carries steep neurological risks.
- The Puberty Shift: Hormonal surges in teenagers naturally block insulin. Expect a temporary wave of insulin resistance and adjust targets compassionately alongside your medical team.
School Tiffin & Meals for a Child with Type 1 Diabetes: Indian Ideas That Work
Sending a child with Type 1 Diabetes (T1D) to school shouldn’t mean packing isolation in a lunchbox. There is no such thing as a restrictive “diabetic diet”—your child can enjoy the same vibrant, traditional Indian meals as their classmates.
The strategy lies in building a metabolic speed bump. Pure carbohydrates spike blood sugar rapidly. However, combining them with proteins and healthy fats slows digestion down, ensuring a steady, stable stream of energy instead of a sharp post-lunch spike.
Following ICMR guidelines, a balanced plate balances 50–55% complex carbs, 15–20% protein, and 25–35% healthy fats.
Smart, Carb-Counted Tiffin Ideas (ISPAD-Aligned)
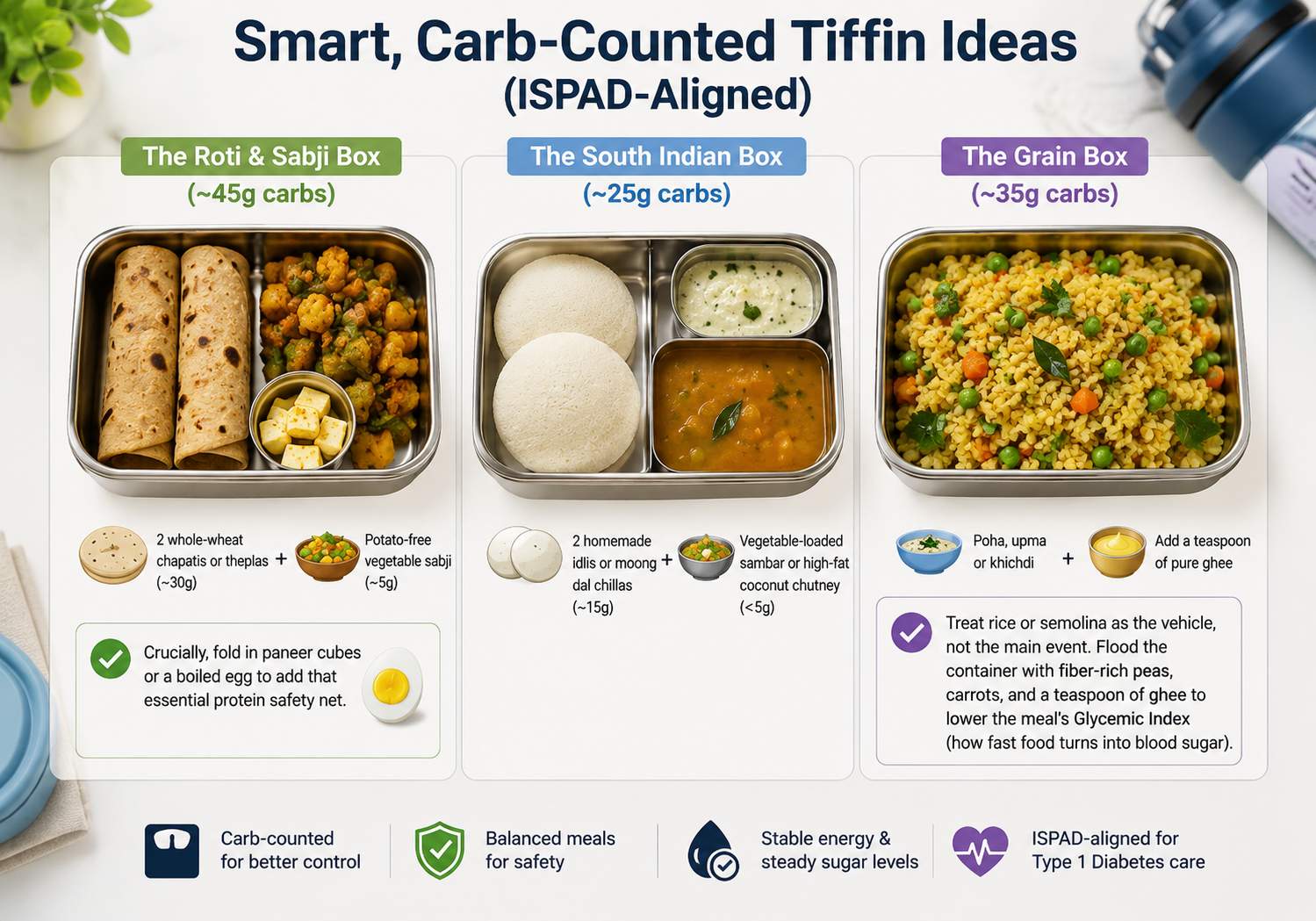
- The Roti & Sabji Box (~45g carbs): Pair 2 whole-wheat chapatis or theplas (~30g) with potato-free vegetable sabji (~5g). Crucially, fold in paneer cubes or a boiled egg to add that essential protein safety net.
- The South Indian Box (~25g carbs): 2 homemade idlis or moong dal chillas (~15g) paired with a vegetable-loaded sambar or high-fat coconut chutney (<5g).
- The Grain Box (~35g carbs): If packing poha, upma, or khichdi, treat rice or semolina as the vehicle, not the main event. Flood the container with fiber-rich peas, carrots, and a teaspoon of pure ghee to lower the meal’s Glycemic Index (how fast food turns into blood sugar).
The Classroom Protection Plan: Work with teachers to ensure your child can pre-bolus (inject mealtime insulin 15–20 minutes before the lunch bell rings). Always leave an explicit, brightly labeled “Low Box” in the classroom containing juice boxes or glucose powder for immediate hypo treatment.
Let your child help count carbs and pick their tiffin box—it turns clinical compliance into a lifelong badge of independence.
How to Talk to Your Child’s School, Teachers & Friends About Type 1 Diabetes
Sending a child with Type 1 Diabetes (T1D) to school can feel daunting, but building a supportive care network ensures their safety and your peace of mind. Think of school staff not just as educators, but as your child’s temporary medical guardians.
1. The ABCD School Action Plan
Instead of a casual chat, establish a reliable protective shield using this structured communication framework before the school term begins:
- Alert: Schedule an intake meeting with the school principal and primary class teacher.
- Build: Work with your pediatric endocrinologist to draft an official care plan detailing blood sugar targets and emergency steps.
- Communicate: Share this document clearly with everyone—from the sports coach to the school bus driver.
- Deliver: Provide the classroom with a highly visible “Low Box” packed with fast-acting glucose powder, juice boxes, and backup testing supplies.
2. Actionable Rules for Teachers
Teachers don’t need a dense medical lecture; they need clear, non-negotiable instructions. Ensure they understand your child requires unrestricted, immediate bathroom and water access, permission to eat snacks mid-lesson to treat a sudden drop, and full inclusion in sports.
3. De-stigmatizing T1D with Classmates
Peers are naturally curious. Partner with the teacher for a quick, 15-minute classroom chat. Demystify the condition by using a doll to demonstrate a simple finger-prick, and emphasize two critical facts: it is completely non-contagious, and it was not caused by eating too many sweets. Always check your child’s comfort level first to protect their personal privacy and emotional boundaries.
Type 1 Diabetes in Teenagers: Puberty, Hormones & Why Blood Sugar Gets Harder
Puberty is a biological storm. If managing childhood diabetes is like driving a car, adolescence turns it into piloting a rocket through turbulence.
The Hormonal Signal Jammer
During teens, surging growth hormone, cortisol, and sex hormones flood the system. These chemicals act like a biological “signal jammer,” causing a massive 30% to 50% jump in insulin resistance. To break through, daily insulin needs manually double—skyrocketing from a childhood baseline of 0.7–0.9 units/kg up to 1.2–2.0 units/kg.
This hormonal wave peaks overnight, causing the “Dawn Phenomenon” (high waking blood sugar). For teenage girls, menstruation adds volatility: blood sugar spikes pre-period and plummets once bleeding begins, raising low blood sugar (hypoglycemia) risks.
Behavioral Risks & The Alcohol Trap
The mental push for independence can trigger dangerous clinical red flags:
- Insulin Purging: Deliberately skipping doses to lose weight, which rapidly accelerates organ damage.
- The Alcohol Trap: Alcohol forces the liver to prioritize processing toxins, completely blocking it from releasing emergency sugar stores (glycogen). This triggers severe, delayed crashes while the teen sleeps.
Chronic high blood sugar can physically delay skeletal maturation and puberty itself. Because physiology is so volatile now, international guidelines urge parents to prioritize empathy over perfect numbers. Support their daily effort, not just the glucometer log.
Government Support & Free Insulin for Children with Type 1 Diabetes in India
Managing a child’s Type 1 Diabetes (T1D) should never mean financial ruin. India carries the world’s highest pediatric T1D burden, but a massive policy shift is building a vital medical safety net for families.
1. The May 2026 National Framework & Free Care
The Union Health Ministry’s newly launched National Framework for Childhood Diabetes Management expands free, grassroots screening from birth to 18 years across government schools and villages. Children diagnosed through this system are promised entirely free lifelong insulin, glucometers, and monitoring strips.
2. State-Level Initiatives & Jan Aushadhi Pharmacies
- State-Level Access: Local government hospitals provide free standard insulins. Progressive states like Goa, Uttarakhand, and West Bengal (partnering with UNICEF) go further, providing expensive, advanced analogue insulins (like Novorapid) completely free.
- Jan Aushadhi Kendras: If state hospitals are out of reach, these government generic pharmacies slash insulin and testing strip prices by 50% to 90%, removing the financial sting.
3. Lifeline NGO Networks
When public channels fall short, robust non-profits fill the gap:
- Changing Diabetes® in Children: Supplies free insulin and monitoring kits to low-resource youth under 25.
- Udaan & Idhayangal Trust: Provide free insulin cartridges, strips, and even specialized medical refrigerators to underprivileged rural households.
FAQ
How many children have type 1 diabetes in India?
India has the highest number of children with Type 1 diabetes globally. An estimated 301,000 children and adolescents under 20 live with the condition. For younger children under 14, there are approximately 95,600 to 100,000 cases.
Free insulin for Type 1 diabetes in India?
Yes, free insulin is available in India. The government’s new national guidelines promise free lifelong insulin for children. State programs, such as in West Bengal, also offer free insulin. Additionally, NGOs like Udaan and Changing Diabetes in Children supply free insulin to underprivileged youth.
Prevalence of diabetes in children in India?
The national prevalence of diabetes in India is 0.94% for school-age children and 0.56% for adolescents. Globally, India holds the highest burden, with approximately 301,000 children and adolescents (under 20) and nearly 100,000 younger children (under 14) currently living with Type 1 diabetes.
Incidence and prevalence of type 1 diabetes in India?
In India, the incidence of Type 1 diabetes is approximately 4.9 cases per 100,000 people annually. Prevalence is the highest globally, with an estimated 941,000 individuals of all ages currently living with the condition, including 301,000 children and adolescents under the age of 20.
What foods should type 1 diabetics avoid?
Type 1 diabetics should avoid highly processed foods, deep-fried items, and bakery products. They must strictly limit sugar-sweetened beverages (like sodas and juices), refined carbohydrates, and foods high in salt, saturated fats, and trans fats.
Reference
https://pubmed.ncbi.nlm.nih.gov/25941646
https://pmc.ncbi.nlm.nih.gov/articles/PMC6177665
https://en.wikipedia.org/wiki/Diabetes_in_India
https://www.diabetes.org.uk/living-with-diabetes/life-with-diabetes/children-and-diabetes/symptoms
https://www.nhs.uk/conditions/type-1-diabetes/symptoms
https://www.diabetes.co.uk/4ts-of-type1-diabetes.html
https://www.diabetes.org.uk/about-diabetes/type-1-diabetes/symptoms
https://link.springer.com/article/10.1007/s13410-015-0441-x
https://pmc.ncbi.nlm.nih.gov/articles/PMC4265883
https://www.ncbi.nlm.nih.gov/books/NBK470282
https://emedicine.medscape.com/article/907111-overview
https://www.rxdx.co.in/pediatrics/articles/insulin_transition_from_iv_to_sc_in_dka_recovery
https://pubmed.ncbi.nlm.nih.gov/24113878
https://www.udaankids.org/about
https://www.breakthrought1d.org/t1d-resources/school
https://pmc.ncbi.nlm.nih.gov/articles/PMC4413396
https://pubmed.ncbi.nlm.nih.gov/30307692
https://www.ncbi.nlm.nih.gov/books/NBK278938
https://pmc.ncbi.nlm.nih.gov/articles/PMC4413396
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC5793337
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4141579
https://kids.idf.org/media/uploads/2025/04/KiDS-English-India-school-pack-2024_compressed.pdf
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11067706
https://pmc.ncbi.nlm.nih.gov/articles/PMC3968718
https://www.bluecircle.foundation/blog/diabetes-budget-india
About the author
It’s me Mohammad Junaid Rain an MBBS student at GMC Nagpur, passionate about making evidence-based medical information accessible to every Indian. “medstuffs.com” is dedicated to clear, disease education for patients and caregivers.
Disclaimer: This article is for educational purposes only and does not substitute professional medical advice. Please consult your doctor for diagnosis and treatment.