

Stepping onto a football pitch or cricket field with Type 1 Diabetes can feel like trying to drive a manual sports car while reading the engine manual in the dark. One minute you’re sprinting for a clean shot; the next, your CGM alarm is screaming, or a sudden burst of pre-game adrenaline sends your blood sugar through the roof.
It is deeply frustrating when the game you love starts to feel like an exhausting, high-stakes math problem. But a T1D diagnosis should never lock you on the benches. Managing sports in type 1 diabetes isn’t about chasing a perfect, flatlined glucose graph—it’s about equipping yourself with a dynamic, predictable playbook.
Whether you are battling the dreaded 30-hour post-match “sponge effect,” trying to outsmart an automated “smart pump” that keeps over-correcting right before kickoff, or mastering the exact science of a sideline 15-15 pit stop, this guide has you covered. We are breaking down the clinical chaos into actionable, step-by-step strategies for before, during, and long after the final whistle blows. Let’s get you off the sidelines and safely back in the zone.
Is It Safe for People with Type 1 Diabetes to Play Cricket, Football & Other Sports?
Absolutely. Engaging in sports in type 1 diabetes is not only safe; it is highly recommended. From local cricket pitches to Olympic stadiums, T1D doesn’t mean sitting on the sidelines.
The Fuel & Brake System: How Your Body Responds
Think of mixed sports like football or cricket as stop-and-go city driving. Unlike steady jogging, which acts like a continuous drain on your glucose tank, these intermittent sports blend moderate movement with explosive sprints.
- The Aerobic Cruise: Continuous jogging enhances insulin sensitivity, allowing muscles to pull glucose directly from the bloodstream.
- The Anaerobic Sprint: Quick bursts of maximum effort trigger a surge of counter-regulatory hormones (like adrenaline and glucagon). This acts like an internal backup generator, temporarily raising blood sugar and protecting you from a sudden crash during active play.
Proactive On-Field Management
Navigating the field requires a strategic game plan to handle common frustrations, from pre-match anxiety spikes to CGM alarms.
- Scan Frequently: Check your glucose trends before, every 30 minutes during, and after the game to intercept drops early.
- Micro-Dose Carbs: Consume 15 to 30 grams of fast-acting carbohydrates for every 30 minutes of exertion, depending on your starting numbers.
- Watch the 30-Hour Tail: Your muscles will actively rebuild glycogen stores for up to 30 hours after the final whistle. Anticipate delayed nighttime lows with a low-glycemic bedtime snack or adjusted basal insulin.
Managing Blood Sugar Before, During & After Cricket or Football Matches
Thriving in high-intensity sports in type 1 diabetes requires treating your metabolism like a finely tuned race car: you need a precise fueling strategy for every lap of the match.
1. Pre-Match: Fueling the Engine
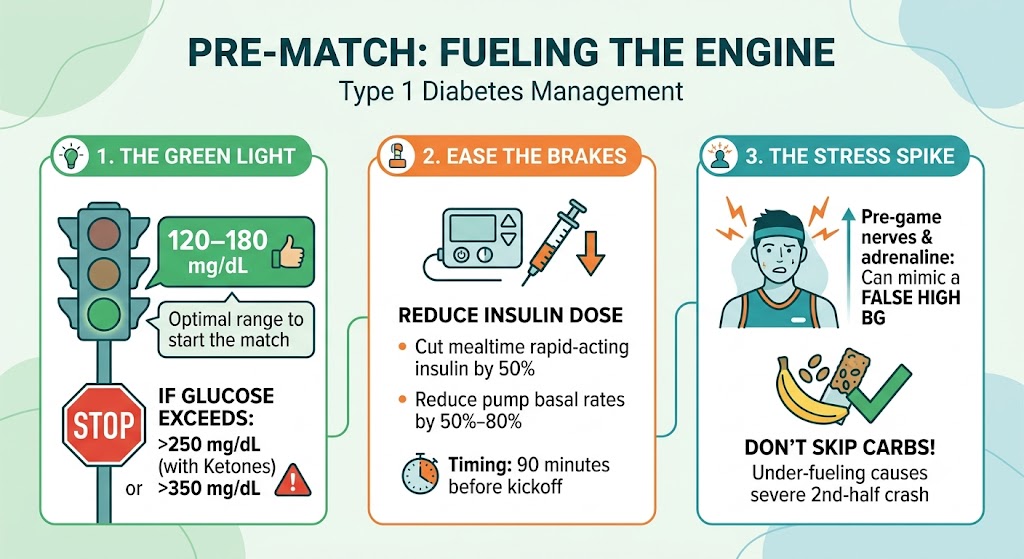
- The Green Light: Target a baseline of 120–180 mg/dL. If glucose exceeds 250 mg/dL with ketones (or 350 mg/dL without), pull into the pit stop and correct it first.
- Ease the Brakes: Cut rapid-acting mealtime insulin by 50%, or reduce pump basal rates by 50%–80% roughly 90 minutes before kickoff.
- The Stress Spike: Pre-game nerves unleash adrenaline, mimicking a false high. Don’t let this trick you into skipping pre-game carbs; under-fueling guarantees a severe second-half crash.
2. In-Game: The Intermittent Advantage
- The Safety Net: The stop-and-go sprints of cricket and football trigger counter-regulatory hormones that prompt the liver to release glucose. This internal backup means you typically need fewer external carbohydrates than endurance runners.
- Tech Check: Scan your CGM every 30 minutes. If you feel low but your screen reads normal, trust your gut and do a finger-stick—CGM sensors can lag during rapid shifts. Fuel with 15–30g of fast carbs per half-hour.
3. Post-Match: The 30-Hour “Sponge Effect”
Once the final whistle blows, your muscles act like a dry sponge, aggressively soaking up blood glucose to rebuild depleted glycogen stores. This extreme insulin sensitivity lasts up to 30 hours, creating a high risk for midnight crashes.
To stay safe, slash your post-match meal insulin by 50% and overnight basal by 20%. Prioritize a low-GI recovery meal, and pair a bedtime snack with protein. If intense anaerobic spikes leave you high immediately after the whistle, correct carefully using 100%–150% of your usual correction factor.
Recognizing & Preventing Hypoglycemia During Practice or Match Play
The Invisible Fuel Leak
When engaging in sports in type 1 diabetes, a massive adrenaline rush acts like a loud car radio—it can easily drown out your body’s internal “low fuel” warning lights. Hypoglycemia (blood sugar below 70 mg/dL) hits athletes in two distinct phases:
- Autonomic Alarms: Shakiness, sweating, and a racing heart.
- Neuroglycopenic Outages: Dizziness, blurred vision, and “brain fog.”
Because intense physical exertion mimics and masks these early warning signs, a crash can sneak up rapidly, impairing your coordination and quick decision-making on the field.
Defensive Strategies on the Pitch
Preventing a low requires setting your metabolic defenses before the whistle blows:
- Audit the Dashboard: Check your glucose every 30 minutes. If you feel symptomatic but your CGM reads normal, do a finger-stick—sensors can lag behind actual capillary drops during high-intensity movement.
- Pre-Match Tweaks: If starting below 90 mg/dL, take 15–30g of fast carbs and delay play. For meals within 3 hours of play, scale back rapid-acting insulin by 50%–75%, or reduce pump basal rates by 50%–80% roughly 90 minutes before kickoff.
The 15-15 Sideline Pit Stop
If you hit a low, pull out of the game immediately and deploy the 15-15 Rule:
- Fuel: Eat 15g of fast-acting carbs. Avoid chocolate or high-fat snacks; fat acts like a traffic jam, slowing down glucose absorption into your bloodstream.
- Pause: Wait 15 minutes, recheck your levels, and repeat if necessary. Once stable, eat a complex carb and protein snack (like cheese and crackers) to keep your tank steady.
Emergency Airbag: For severe drops (<55 mg/dL) where fainting occurs, glucagon is your ultimate safety net. Always keep an injectable or nasal glucagon kit in your sports bag, and ensure your coach or a teammate knows exactly how to use it.
Pre-Game Nutrition, Carb Timing & Hydration for Young Diabetic Athletes
Mastering sports in type 1 diabetes requires perfectly sync’ing pre-game nutrition with active insulin. Think of dietary carbohydrates like firewood: low-glycemic index (GI) foods act like a slow-burning oak log providing sustained energy for long matches, while high-GI fast carbs are like lighter fluid—perfect for quick bursts of energy.
The Pre-Game Blood Sugar Dashboard
Before stepping onto the pitch, your current blood glucose (BG) dictates your immediate metabolic strategy:
- Below 90 mg/dL: Take 15–30g of fast carbs (or 0.3–0.5 g/kg). Delay play until BG crosses 90 mg/dL.
- 90–149 mg/dL: Eat a low-GI snack (0.5–1.0 g/kg) mixed with protein/fat (like yogurt or milk) at kickoff for stable fueling. Try adding fructose (fruit) 30 minutes prior for a steady liver glucose release.
- 150–249 mg/dL: Safe to play. Hold off on extra carbs until levels drop below 150 mg/dL.
- Above 250 mg/dL: Check ketones. If present, or if BG exceeds 350 mg/dL, bench the athlete and administer corrective insulin to avoid metabolic distress.
Outsmarting the “Smart Pump” Trap
For athletes using Automated Insulin Delivery (AID) systems, a major tech frustration is timing. If a young athlete eats a pre-game snack too early, the pump’s algorithm detects rising blood sugar and automatically injects a corrective insulin dose. This leaves the athlete with high “insulin on board” right at kickoff, triggering an immediate hypoglycemic crash.
To prevent this, give pre-game meals 1–3 hours before the match, paired with a 50%–75% reduction in rapid-acting mealtime insulin.
Hydration is the Lubricant
Dehydration acts like a stressor on the body, triggering cortisol releases that cause unpredictable blood sugar spikes. Ensure regular water intake, or substitute with electrolyte-rich sports drinks if you need to actively rescue dropping glucose levels.
Insulin Dose Adjustments for Sports Days: Pump & Injection Strategies
Managing active insulin during sports in type 1 diabetes is like loosening the brakes on a bicycle before a steep descent. If your “brakes” (circulating insulin) are applied too firmly, you risk a grinding hypoglycemic halt on the field.
Multiple Daily Injections (MDI) Tactics
- The Pre-Game Cut: For intermittent sports like football or cricket, scale back your rapid-acting meal bolus by 50% if eating within 3 hours of play.
- Guard Your Injection Sites: Stick to the abdomen. Avoid injecting into active muscle groups (like the thighs) right before running. Increased localized blood flow acts like an express elevator, rushing insulin into your bloodstream and triggering a rapid crash.
- Tournament Basals: For all-day events, reduce your background basal insulin by 20%–50%.
Insulin Pump Adjustments
- Proactive Temporary Basal Rates (TBR): Reduce your basal rate by 50%–80% roughly 90 minutes before the whistle blows to clear out circulating insulin in time for kickoff.
- The Disconnection Limit: If disconnecting the pump for contact sports, cap your off-line time at a strict maximum of 90 minutes to avoid rebound hyperglycemia or ketone accumulation.
Post-Game Recovery
Your muscles remain highly insulin-sensitive long after the match ends. To prevent delayed midnight crashes, cut your post-match meal bolus by 50% [Insert Citation]. Before bed, consume a low-GI snack paired with protein without taking a covering bolus, and lower your overnight basal rate by 10%–20%.
Resources
https://pubmed.ncbi.nlm.nih.gov/23897688
https://pubmed.ncbi.nlm.nih.gov/40036800
https://pmc.ncbi.nlm.nih.gov/articles/PMC6768890
https://pmc.ncbi.nlm.nih.gov/articles/PMC5520333
https://pubmed.ncbi.nlm.nih.gov/20807120
https://pubmed.ncbi.nlm.nih.gov/33047169
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6950062
https://pmc.ncbi.nlm.nih.gov/articles/PMC8942069
https://pubmed.ncbi.nlm.nih.gov/27168135
https://pubmed.ncbi.nlm.nih.gov/16918069
https://nin.res.in/dietaryguidelines/pdfjs/locale/DGI_2024.pdf
About the Author
It’s me Mohammad Junaid Rain an MBBS student at GMC Nagpur, passionate about making evidence-based medical information accessible to every Indian. “medstuffs.com” is dedicated to clear, disease education for patients and caregivers.
Disclaimer: This article is for educational purposes only and does not substitute professional medical advice. Please consult your doctor for diagnosis and treatment.