
If you or someone in your family has Type 2 diabetes, you have probably heard your doctor say — “Let’s start you on some medication.”
And your first reaction might have been — “But I am already dieting and walking every day. Why do I still need medicine?”
You are not alone. This is one of the most common questions diabetic patients ask.
The truth is — Type 2 diabetes medications are not a sign of failure. They are a tool. And understanding them can actually help you take better control of your condition.
In this guide, we will break down the complete type 2 diabetes medications list — from the most commonly prescribed Metformin to the newest 2025 drug Tirzepatide — in simple, everyday language that anyone can understand.
Why medication is often needed alongside lifestyle changes
You have been eating less carbs. You go for a morning walk. You avoided sweets at the last family function. So why is your doctor still writing a prescription?
Here is the honest answer — lifestyle changes alone are often not enough.
Type 2 diabetes is a progressive condition. Over time, your pancreas gets tired. It produces less and less insulin. No matter how disciplined your diet is, a weakened pancreas cannot keep up with your body’s demand for insulin on its own.
From My Medical Studies “In our pharmacology classes, we learn that Type 2 diabetes is not just a lifestyle disease — it is also a disease of progressive beta-cell failure because of overwork on beta cell of pancreas. Even the most disciplined patient will eventually need medication because the pancreas itself is losing its ability to produce enough insulin. This is not the patient’s fault. It is the natural history of the disease.” — Mohammad Junaid Rain, MBBS 2nd Year
According to the 2024 ADA and AACE Guidelines, diet and lifestyle changes can help improve blood sugar levels — but pharmacologic (medicine-based) intervention is usually necessary for adequate long-term control in most patients.
Think of it this way — lifestyle changes slow down the problem. Medication helps fix it from the inside.
The goal is never to stay on medication forever. For many patients, getting blood sugar under control with medication first — then working on lifestyle — actually gives better long-term results than lifestyle alone.
References:
- ADA + AACE Pharmacologic Recommendations 2024 — University of Illinois Chicago
- Common Crossroads in Diabetes Management — PMC
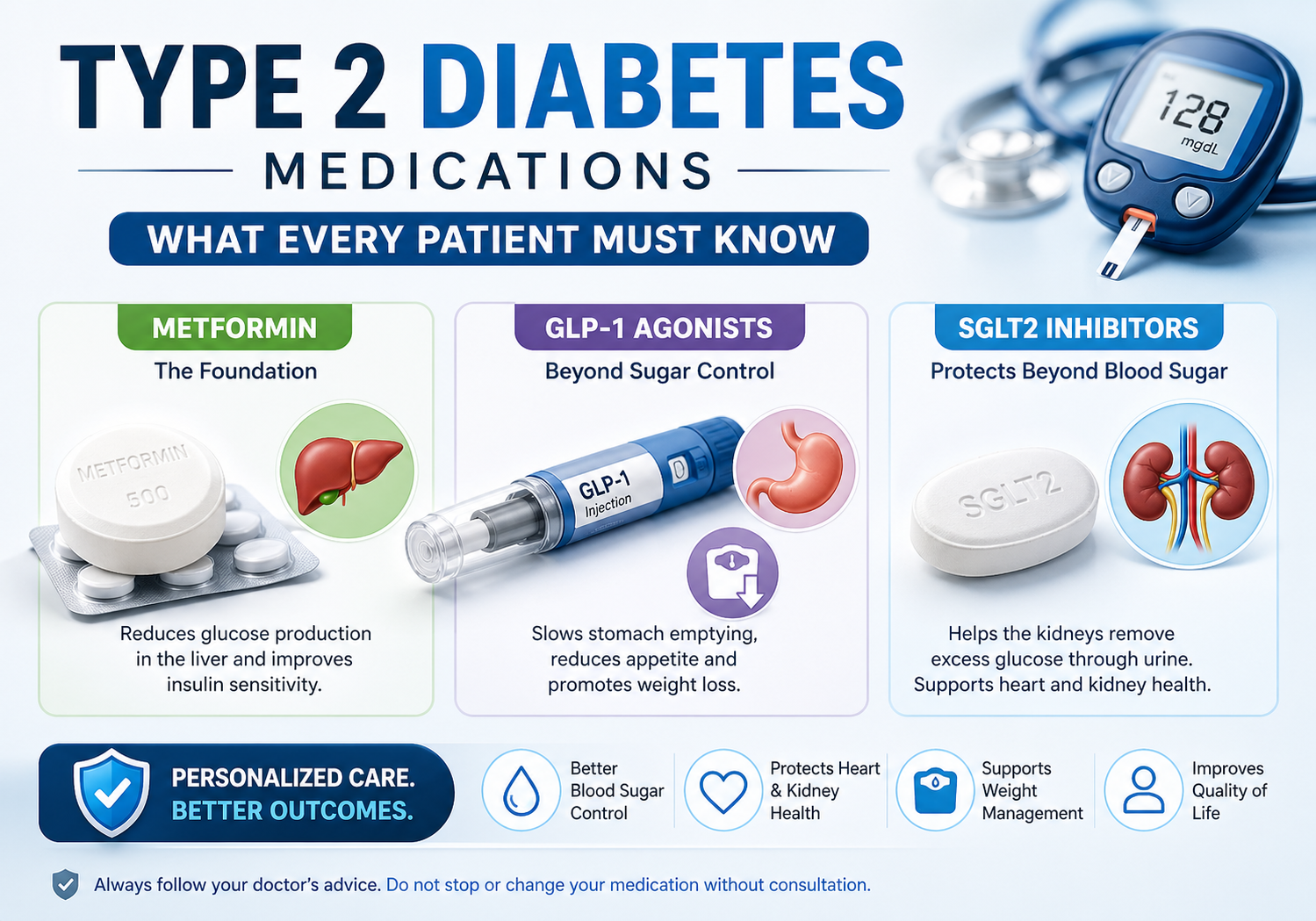
Metformin – how it works, side effects, who it’s for
If you have been recently diagnosed with Type 2 diabetes in India, there is a very high chance your doctor handed you a prescription with one name on it — Metformin.
Sold in India as Glycomet, Glucophage, or Obimet, Metformin is the most prescribed diabetes drug in the world. More than 200 million people take it every single day.
But what exactly does it do inside your body?
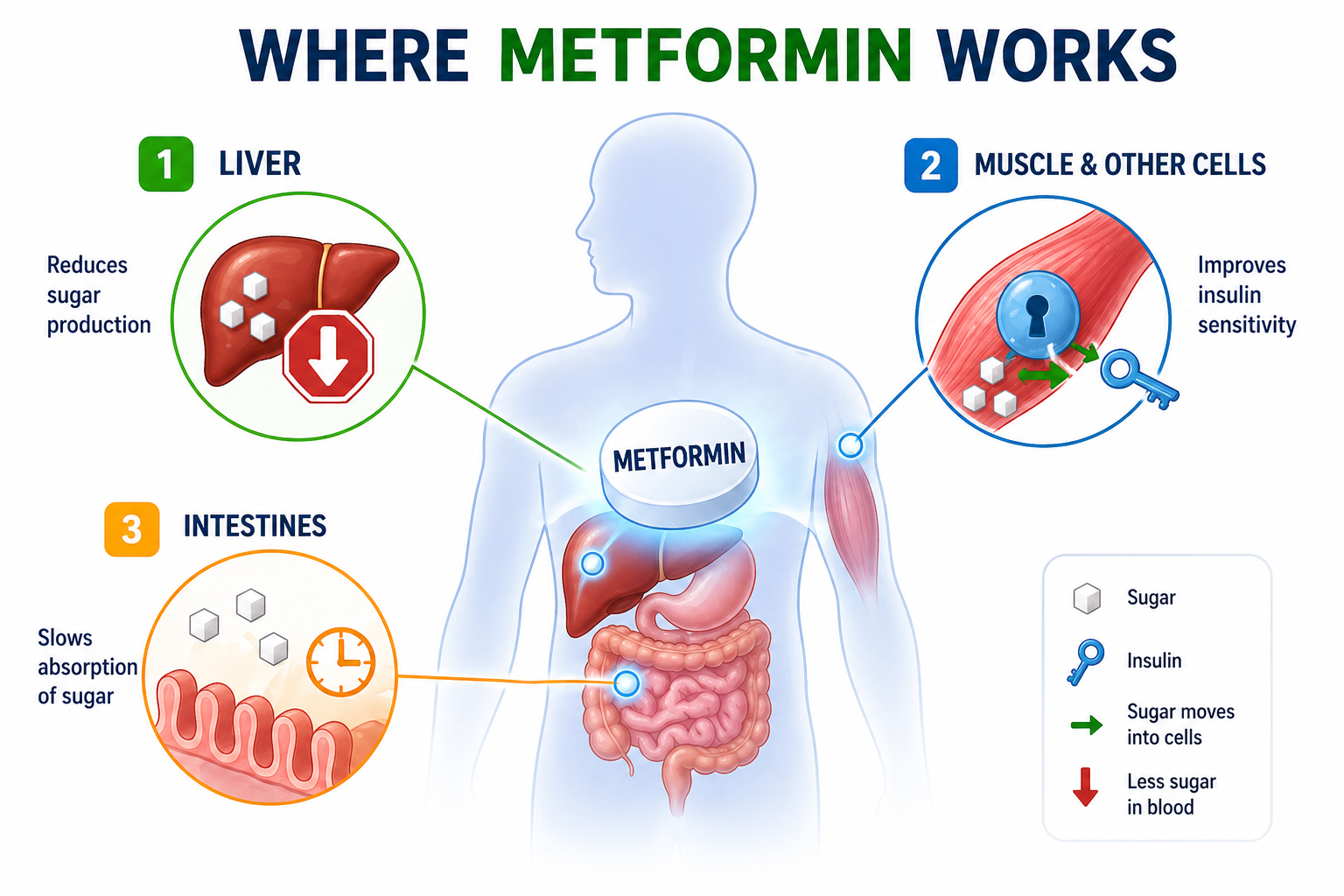
How Metformin Works — Simply Explained
Think of your liver like an overenthusiastic cook. Even when you have not eaten anything, your liver keeps releasing sugar into your blood — unnecessarily. In Type 2 diabetes, this problem gets worse.
Metformin’s main job is to tell that cook to calm down.
It works in 3 simple ways:
1. Stops the liver from releasing excess sugar — This is its most important action. Even while you sleep, Metformin is quietly reducing your fasting blood sugar.
2. Makes your body’s cells more sensitive to insulin — Your cells start responding better to insulin, so sugar moves out of blood and into cells more efficiently.
3. Slows sugar absorption from food — It slightly slows how fast sugar from your meal enters your bloodstream, preventing sudden spikes after eating.
From My Medical Studies “In our pharmacology class, Metformin falls under the biguanide class of drugs. What genuinely surprised me when I first studied it — despite being used for over 60 years and taken by 200 million people daily, scientists still do not fully understand every mechanism through which it works. It acts on the liver, the gut, the gut microbiome, and even immune cells. It is one of the most fascinating drugs in our entire pharmacology syllabus.” — Mohammad Junaid Rain, MBBS 2nd Year
Who Should Take Metformin?
According to the American Diabetes Association 2024 Guidelines, Metformin is the preferred first-line medication for Type 2 diabetes in most adults — especially those who are:
- Newly diagnosed with Type 2 diabetes
- Overweight or obese
- Have HbA1c between 7–9%
- Do not have severe kidney disease
Side Effects — What Indians Commonly Experience
Metformin is generally very safe. But it does have some common side effects — especially in the beginning:
| Side Effect | How Common | What To Do |
|---|---|---|
| Nausea | Very common | Take with food — not on empty stomach |
| Loose motions / Diarrhea | Common | Usually settles in 2 weeks |
| Stomach discomfort | Common | Start with low dose, increase slowly |
| Metallic taste | Occasional | Usually temporary |
| Vitamin B12 deficiency | Long-term use | Ask doctor to check B12 yearly |
Important: Metformin does not cause low blood sugar (hypoglycemia) on its own. This makes it one of the safest diabetes drugs available.
Who Should NOT Take Metformin?
- People with severe kidney disease (eGFR below 30)
- People with serious liver disease
- Before surgery or contrast dye procedures — doctor will temporarily stop it
References:
- Metformin — StatPearls, NIH Bookshelf
- Metformin: Update on Mechanisms of Action — Nature Reviews Endocrinology
- Metformin Action in the GI Tract — Frontiers in Pharmacology 2024
GLP-1 Receptor Agonists — Ozempic, Trulicity, Victoza Explained
You may have seen Ozempic trending on social media recently — celebrities using it for weight loss, news articles calling it a “miracle drug.”
But what exactly is it? And is it relevant for diabetic patients?
Let’s break it down simply.
What Are GLP-1 Receptor Agonists?
GLP-1 stands for Glucagon-Like Peptide-1. That’s a mouthful — so let’s forget the name and focus on what it does.
Normally, when you eat food, your gut releases a hormone called GLP-1. This hormone does 3 important things:
- Tells your pancreas — “Food has arrived, release insulin now”
- Tells your liver — “Stop releasing extra sugar”
- Tells your brain — “You are full, stop eating”
In Type 2 diabetes, this GLP-1 response becomes weak and sluggish.
GLP-1 receptor agonist drugs are designed to replace and supercharge this missing hormone.
Think of it like this — your body’s natural signal became a whisper. These drugs turn it back into a loud, clear voice.
Common GLP-1 Drugs You Will Hear About
| Brand Name | Generic Name | How Taken | Frequency |
|---|---|---|---|
| Ozempic | Semaglutide | Injection | Once weekly |
| Trulicity | Dulaglutide | Injection | Once weekly |
| Victoza | Liraglutide | Injection | Once daily |
| Rybelsus | Semaglutide | Tablet | Once daily |
Indian Note: Dulaglutide (Trulicity) and Liraglutide (Victoza) are available in India. Ozempic availability has been limited in India — your doctor will guide you on what’s accessible locally.
What Makes GLP-1 Drugs Special?
Unlike older diabetes medicines, GLP-1 drugs do something remarkable — they cause weight loss.
For diabetic patients who are overweight — which is most of them — this is a game changer.
According to a 2024 Lancet review, GLP-1 receptor agonists demonstrated significant efficacy in blood glucose management, weight reduction, cardiovascular disease prevention, and kidney health improvement — all in one drug.
That means one injection per week can simultaneously:
- Lower your HbA1c
- Reduce your weight
- Protect your heart
- Protect your kidneys
Do They Cause Low Blood Sugar?
No — not on their own. GLP-1 drugs are glucose-dependent. They only release insulin when blood sugar is actually high. When blood sugar is normal, they stop working automatically.
This makes them much safer than older drugs like sulfonylureas.
🩺 From My Medical Studies “In our physiology classes, we study the incretin effect — how gut hormones like GLP-1 and GIP amplify insulin release after meals. What is remarkable about GLP-1 receptor agonist drugs is that they mimic this natural incretin hormone so precisely that the pancreas only responds when blood sugar is actually elevated. This glucose-dependent mechanism is what makes them so safe — your blood sugar cannot crash because the drug automatically switches off at normal glucose levels. As a student, learning about this mechanism genuinely changed how I think about diabetes treatment.” — Mohammad Junaid Rain, MBBS 2nd Year.
Side Effects of GLP-1 Drugs
The most common side effects are gut-related — because GLP-1 slows down digestion deliberately:
| Side Effect | How Common | Tips |
|---|---|---|
| Nausea | Very common initially | Starts low dose, increases slowly |
| Vomiting | Occasional | Usually improves after 4 weeks |
| Loss of appetite | Common | Actually helpful for weight loss |
| Diarrhea or constipation | Occasional | Stay well hydrated |
Important: These side effects are usually temporary — worst in the first 2–4 weeks, then significantly improve.
Who Is This Drug For?
GLP-1 receptor agonists are ideal for Type 2 diabetic patients who:
- Have not achieved target HbA1c on Metformin alone
- Are overweight or obese
- Have existing heart disease or high cardiovascular risk
- Want to avoid injecting insulin
Are They Available and Affordable in India?
Honest answer — currently expensive. Monthly cost can range from ₹3,000 to ₹8,000+ in India depending on the drug and dose. However, prices are gradually coming down as more brands enter the Indian market.
Always discuss cost and availability with your doctor before starting.
References:
- GLP-1 Single, Dual, and Triple Receptor Agonists — The Lancet eClinicalMedicine 2024
- GLP-1 Receptor Agonists — State of the Art — PMC
- Emerging Frontiers in GLP-1 Therapeutics 2025 — PMC
SGLT2 Inhibitors — Jardiance & Farxiga: The Diabetes Drug That Protects Your Heart and Kidneys
Here is something remarkable.
A drug was originally created just to lower blood sugar. But during large clinical trials, researchers noticed something unexpected — patients were having fewer heart attacks, fewer heart failure hospitalizations, and their kidneys were staying healthier for longer.
Scientists were so surprised they ran the trials again. Same result.
That drug was an SGLT2 inhibitor.
Today, these drugs are considered one of the biggest breakthroughs in diabetes treatment in the last 20 years — not because of how well they lower blood sugar, but because of what else they protect.
What Does SGLT2 Even Mean?
SGLT2 stands for Sodium-Glucose Cotransporter 2.
Ignore the complicated name. Here is what it means in simple language:
Your kidneys filter your blood all day. Normally, when sugar passes through the kidney filter, a tiny pump called SGLT2 grabs that sugar and pulls it back into your blood — so it doesn’t get wasted in urine.
In diabetes, this is a problem. You already have too much sugar in your blood. You don’t need it being pulled back in.
SGLT2 inhibitor drugs block that pump.
The result — excess sugar gets flushed out through your urine every single day. Your blood sugar drops without involving insulin at all.
Think of it like this — your kidney becomes a sugar drain.
From My Medical Studies “In our renal physiology lectures, we study how the proximal convoluted tubule reabsorbs almost 90% of filtered glucose through SGLT2 transporters. When I first learned about SGLT2 inhibitors in pharmacology, what struck me was the elegance of the mechanism — instead of forcing the pancreas to produce more insulin or making cells more sensitive, these drugs simply make the kidney excrete the excess sugar. It is a completely different approach to diabetes treatment. And the cardiovascular and kidney benefits discovered later were genuinely unexpected — even for researchers.” — Mohammad Junaid Rain, MBBS 2nd Year
Common SGLT2 Inhibitor Drugs
| Brand Name | Generic Name | Available in India |
|---|---|---|
| Jardiance | Empagliflozin | ✅ Yes |
| Farxiga / Forxiga | Dapagliflozin | ✅ Yes |
| Invokana | Canagliflozin | Limited |
The Heart Benefits — What the Research Actually Shows
This is where SGLT2 inhibitors become truly remarkable.
According to a 2024 PMC cardiovascular outcomes study, SGLT2 inhibitors reduce:
- Risk of cardiovascular death or heart failure hospitalization by 23%
- Risk of kidney disease progression by 45%
- Blood pressure — by 3–5 mmHg systolic
- Body weight — by 2–3 kg on average
For Indian diabetic patients — who already have some of the highest rates of heart disease in the world — these numbers are extremely significant.
The Kidney Benefits — Why Nephrologists Love This Drug
Diabetes is the number one cause of kidney failure in India.
Over time, high blood sugar damages the tiny blood vessels inside the kidneys. Once kidney damage starts, it is very difficult to reverse.
SGLT2 inhibitors slow this damage down significantly. They reduce pressure inside the kidney’s filtering units (glomeruli), reduce inflammation, and protect kidney function over the long term.
In fact, Dapagliflozin (Farxiga/Forxiga) has now been approved specifically for chronic kidney disease — even in patients without diabetes. That is how strong the kidney protection evidence is.
What Else Do SGLT2 Inhibitors Do?
Beyond heart and kidneys, these drugs also:
- Cause mild weight loss — 2–3 kg on average
- Lower blood pressure — without a separate BP medication
- Reduce fatty liver — common in Indian diabetic patients
- Lower uric acid — helpful for patients with gout
Side Effects — What to Watch For
| Side Effect | Why It Happens | What to Do |
|---|---|---|
| Genital fungal infection | Sugar in urine feeds fungus | Maintain good hygiene, inform doctor |
| Increased urination | Kidney flushing sugar | Expected — drink more water |
| UTI (Urinary Tract Infection) | More common in women | Stay hydrated, inform doctor early |
| Dehydration | Fluid loss with sugar | Drink adequate water daily |
| DKA (rare but serious) | Especially if insulin stopped suddenly | Never stop insulin without doctor’s advice |
Important Warning: SGLT2 inhibitors should be stopped 3 days before any surgery or major illness. They can cause a dangerous condition called euglycemic DKA — where blood sugar appears normal but the body is in ketoacidosis. Always inform your surgeon if you are taking these drugs.
Who Is This Drug Best For?
SGLT2 inhibitors are ideal for Type 2 diabetic patients who:
- Have existing heart disease or heart failure
- Have early kidney disease (CKD stage 1–3)
- Are overweight and need mild weight reduction
- Have high blood pressure alongside diabetes
- Want to avoid insulin for as long as possible
Who Should NOT Take SGLT2 Inhibitors?
- Patients with severe kidney disease (eGFR below 20–30)
- Patients with recurrent UTIs or fungal infections
- Type 1 diabetes patients (unless specifically prescribed)
- Pregnant women
References:
- Protective Influence of SGLT-2 Inhibitors Against Heart Failure — PMC 2024
- Clinical Evidence for Cardiovascular & Kidney Benefits — PMC
- SGLT2 Inhibitors: Antidiabetic and Cardioprotective Effects — PMC
- Emerging Horizons: SGLT-2 Inhibitors Beyond Diabetes — PMC
DPP-4 inhibitors, sulfonylureas, TZDs
So far we have covered the star players — Metformin, GLP-1 agonists, and SGLT2 inhibitors.
But your doctor’s prescription might contain other names you don’t recognise — words like Glipizide, Januvia, Pioglitazone, or Glimepiride.
These belong to three older but still widely used drug classes. They are not as glamorous as Ozempic. But for millions of diabetic patients — especially those who cannot afford newer drugs — these medicines are the backbone of daily diabetes management.
Let’s understand each one.
Part 1 — DPP-4 Inhibitors (Gliptins)
Common names: Sitagliptin (Januvia), Vildagliptin (Galvus), Saxagliptin (Onglyza)
Indian brands: Januvia, Galvus, Zita, Istavel
Remember GLP-1 — the gut hormone we discussed in the previous section? Your body naturally produces it after meals. But there is a problem — an enzyme called DPP-4 destroys GLP-1 within just 2 minutes of it being released.
DPP-4 inhibitors block that destroying enzyme.
The result — your natural GLP-1 survives longer, works better, and helps control blood sugar more effectively after meals.
Think of it like this — GLP-1 is a hardworking employee. DPP-4 is a manager who fires them too quickly. DPP-4 inhibitors remove that manager.
From My Medical Studies “In pharmacology, we classify DPP-4 inhibitors as incretin enhancers — they don’t add a new hormone, they simply protect the one your body already makes. What I find clinically interesting is how gentle these drugs are. They have almost no risk of hypoglycemia, cause no weight gain, and are well tolerated even in elderly patients. In India, where many diabetic patients are elderly and managing multiple conditions, this makes gliptins a very practical choice.” — Mohammad Junaid Rain, MBBS 2nd Year
Key advantages of DPP-4 inhibitors:
- No hypoglycemia risk
- No weight gain — weight neutral
- Once daily tablet — simple to take
- Safe for elderly patients
- Can be used with kidney disease (dose adjustment needed)
Limitations:
- Moderate glucose lowering — not the strongest drug
- More expensive than sulfonylureas
- Rare risk of joint pain and pancreatitis
Part 2 — Sulfonylureas
Common names: Glimepiride, Glipizide, Gliclazide, Glibenclamide
Indian brands: Amaryl, Glynase, Diamicron, Daonil
Sulfonylureas are the oldest class of oral diabetes drugs — used since the 1950s. They are extremely cheap, widely available across every pharmacy in India, and highly effective at lowering blood sugar quickly.
How they work:
Your pancreas has beta cells that produce insulin. Sulfonylureas directly knock on those beta cells and say — “Produce more insulin. Now. Regardless of blood sugar level.”
This is both their strength and their biggest weakness.
From My Medical Studies “In our pharmacology viva, sulfonylureas always come up because of their hypoglycemia risk. Unlike GLP-1 drugs that only work when blood sugar is high, sulfonylureas stimulate insulin release regardless of current blood sugar levels. This means if a patient skips a meal or exercises more than usual, blood sugar can drop dangerously low. As future doctors, we are taught to always warn patients on sulfonylureas about hypoglycemia symptoms — shakiness, sweating, confusion — and to always carry sugar with them.” — Mohammad Junaid Rain, MBBS 2nd Year
Key advantages of Sulfonylureas:
- Very affordable — ₹30–100/month in India
- Available everywhere — even in small town pharmacies
- Strong blood sugar lowering effect
- Decades of safety data
Key disadvantages:
- Hypoglycemia risk — can cause dangerous low blood sugar
- Weight gain — 2–4 kg on average
- Beta cell burnout — with long term use, pancreas gets more exhausted
- Not ideal for elderly patients or those who skip meals
Hypoglycemia warning signs to tell your patients:
| Symptom | What It Means |
|---|---|
| Sudden sweating | Blood sugar dropping |
| Shakiness or trembling | Body releasing adrenaline |
| Confusion or dizziness | Brain not getting enough glucose |
| Extreme hunger suddenly | Body signalling emergency |
| Pale skin | Reduced blood flow |
What to do: Immediately eat 2–3 teaspoons of sugar or drink a glass of fruit juice. Then eat a proper meal.
Part 3 — TZDs (Thiazolidinediones / Glitazones)
Common name: Pioglitazone
Indian brands: Pioz, Actos, Glita
TZDs work in a completely different way from all the drugs above.
Instead of targeting the pancreas or kidney — they go directly into your fat cells and muscle cells and make them more sensitive to insulin.
Think of it like this — insulin is knocking on the door of your cells. In Type 2 diabetes, cells are not answering the door. Pioglitazone makes the cells open the door properly.
Key advantages of Pioglitazone:
- Reduces insulin resistance at the root level
- Helps with non-alcoholic fatty liver disease — very relevant for Indians
- Cardioprotective effects in some patients
Key disadvantages and warnings:
| Concern | Detail |
|---|---|
| Weight gain | 3–5 kg fluid retention |
| Swelling in legs | Fluid accumulation — common |
| Heart failure risk | Avoid in patients with heart failure |
| Bone fracture risk | Long term use — especially in women |
| Bladder cancer concern | Very rare — discuss with doctor if long term use |
Important: Pioglitazone should be avoided in patients with heart failure, active bladder problems, or liver disease.
Quick Comparison — All Three Drug Classes
| Feature | DPP-4 Inhibitors | Sulfonylureas | TZDs |
|---|---|---|---|
| Hypoglycemia risk | Very low | High | Low |
| Weight effect | Neutral | Weight gain | Weight gain |
| Cost in India | Moderate | Very cheap | Cheap |
| Heart benefit | Neutral | Neutral | Some benefit |
| Best for | Elderly patients | Budget-conscious | Insulin resistance |
| Common Indian brand | Galvus, Januvia | Amaryl, Glynase | Pioz, Glita |
References:
- ADA + AACE Pharmacologic Recommendations 2024 — UIC Drug Information
- 2024 ADA Standards of Care Update — Endocrinology Advisor
- Metformin StatPearls — Combination Therapy Hierarchy — NIH
Dual GLP-1/GIP Agonists — Mounjaro (Tirzepatide): The Newest Diabetes Drug
Let’s talk about the most exciting development in diabetes treatment in the last decade.
In 2022, a new drug called Tirzepatide — sold under the brand name Mounjaro — was approved by the FDA. And the diabetes world has not been the same since.
Why? Because it does something no diabetes drug has ever done before.
Every drug we have discussed so far targets one pathway. Metformin targets the liver. GLP-1 drugs target one hormone. SGLT2 inhibitors target the kidney pump.
Tirzepatide targets two hormones simultaneously — GLP-1 and GIP.
And the results from clinical trials have been, frankly, extraordinary.
What is GIP — The Second Hormone?
You already know GLP-1 from our previous section — the gut hormone that tells your pancreas to release insulin after meals.
GIP stands for Glucose-Dependent Insulinotropic Polypeptide. Another long name — but a simple concept.
GIP is the older sibling of GLP-1. It was actually discovered first. It also stimulates insulin release after meals — but through a completely different pathway in the pancreas.
Think of it like this:
- GLP-1 is one musician playing a song
- GIP is a second musician playing a different instrument
- Tirzepatide combines both musicians into one band — the result is louder, stronger, and more effective
When both hormones are activated together, the insulin response is significantly more powerful than either hormone alone.
From My Medical Studies “In our physiology classes, we study both GLP-1 and GIP as the two main incretin hormones responsible for the incretin effect — the phenomenon where oral glucose causes a much greater insulin response than intravenous glucose. For years, GIP was actually considered less useful in Type 2 diabetes because diabetic patients seemed resistant to its effects. Tirzepatide challenged this assumption entirely. By activating both receptors simultaneously, it appears to restore GIP sensitivity in diabetic patients — something researchers did not expect. As a medical student, this is one of those moments in pharmacology where you realise medicine is still full of surprises.” — Mohammad Junaid Rain, MBBS 2nd Year
What Makes Tirzepatide Results So Remarkable?
Let’s look at the actual numbers from the SURPASS clinical trial program — the largest trials ever done on a diabetes drug:
| Outcome | Tirzepatide Result |
|---|---|
| HbA1c reduction | Up to 2.4% reduction |
| Weight loss | Up to 11.3 kg on 15mg dose |
| Patients reaching HbA1c below 7% | Over 90% on highest dose |
| Comparison vs Semaglutide (Ozempic) | Superior on both HbA1c and weight |
To put this in perspective — most diabetes drugs reduce HbA1c by 0.5–1%. Tirzepatide reduces it by up to 2.4%. That is genuinely unprecedented.
And the weight loss of 11+ kg rivals some bariatric surgery outcomes.
How is Tirzepatide Different From Ozempic?
This is the question everyone asks. Both are weekly injections. Both cause weight loss. Both lower blood sugar.
| Feature | Ozempic (Semaglutide) | Mounjaro (Tirzepatide) |
|---|---|---|
| Hormones targeted | GLP-1 only | GLP-1 + GIP both |
| HbA1c reduction | Up to 1.8% | Up to 2.4% |
| Weight loss | Up to 6–7 kg | Up to 11–13 kg |
| Cardiovascular evidence | Strong — proven | Growing — promising |
| FDA approval | 2017 | 2022 |
| Available in India | Limited | Very limited currently |
Real-world data published in PMC 2025 confirms that tirzepatide outperformed semaglutide on both HbA1c reduction and weight loss in head-to-head comparisons in actual patients — not just clinical trials.
What Are the Side Effects?
Because Tirzepatide works on GLP-1 — which slows digestion — its side effects are very similar to other GLP-1 drugs:
| Side Effect | How Common | Duration |
|---|---|---|
| Nausea | Very common | Worst in first 4 weeks |
| Vomiting | Occasional | Improves with time |
| Diarrhea | Occasional | Usually temporary |
| Constipation | Occasional | Stay hydrated |
| Decreased appetite | Common | Actually beneficial |
| Injection site reaction | Occasional | Rotate injection sites |
The good news — tirzepatide does not cause hypoglycemia on its own. Like GLP-1 drugs, it only works when blood sugar is actually elevated.
Who is Tirzepatide Best For?
Tirzepatide is ideal for Type 2 diabetic patients who:
- Have very high HbA1c — above 9–10%
- Are significantly overweight or obese
- Have failed multiple other medications
- Want to avoid or delay insulin therapy
- Can afford the higher cost
A Word of Caution
Tirzepatide is powerful. But it is not magic. It still works best alongside a healthy diet and regular exercise.
Also — because it is so new, long-term safety data beyond 3–4 years is still being collected. Your doctor will weigh benefits vs risks based on your individual situation.
Reference
Tirzepatide’s Therapeutic Spectrum: Dual GIP/GLP-1 — PMC 2025
Real-World Tirzepatide vs Semaglutide — PMC 2025
Tirzepatide Improves Beta-Cell Function — PMC
When Insulin is Needed & Types of Insulin
For many Indian patients, the word “insulin” brings fear. “Doctor ne bola insulin lena padega” — and the whole family gets worried.
But here is the truth — insulin is not a punishment. It is not a last resort. It is simply replacing what your own pancreas can no longer make enough of.
Type 2 diabetes is progressive. Over years, your beta cells get exhausted. Tablets and injections can only do so much. When HbA1c remains very high despite multiple medications — insulin becomes necessary.
🩺 From My Medical Studies “In our clinical postings, we regularly see patients who delayed insulin for years out of fear. During those years, silent damage continued in their kidneys, eyes and nerves. When they finally started insulin, most said — ‘Doctor, I feel so much better. Why didn’t I start earlier?’ The fear of the needle is almost always worse than the needle itself.” — Mohammad Junaid Rain, MBBS 2nd Year
There are several types of insulin — rapid-acting, short-acting, long-acting, and premixed — each working differently in your body.
We are discussing the insulin in a separate article.
Conclusion
Type 2 diabetes medications can feel overwhelming at first — so many names, so many options.
But now you understand the full picture:
- Metformin — the trusted first step
- GLP-1 agonists — weight loss + blood sugar control
- SGLT2 inhibitors — protect your heart and kidneys
- DPP-4, Sulfonylureas, TZDs — supporting medicines for different needs
- Tirzepatide — the powerful new option of 2025
- Insulin — not a last resort, but a natural and effective treatment
Remember — no medication works alone. Every drug in this list works better when combined with a healthy Indian diet, regular physical activity, and consistent monitoring.
Always work with your doctor to find the combination that is right for your specific situation. Never start, stop, or change any diabetes medication on your own.
This article is for educational purposes only. Please consult your doctor or endocrinologist before making any changes to your diabetes treatment plan.
Q1. What is the first medicine given for Type 2 diabetes?
Metformin is almost always the first medication prescribed for Type 2 diabetes, as recommended by both ADA and RSSDI Indian guidelines.
Q2. What is the best medication for type 2 diabetes?
There is no single “best” medication for Type 2 diabetes — because the right medicine depends on your individual situation.
For most Indian patients — Metformin remains the safest, most affordable and most effective starting point.
But the best medication is always the one your doctor prescribes after evaluating your HbA1c, weight, kidney function, heart health and budget.
Never self-medicate. Always consult your doctor
Q3. Which diabetes medicine causes weight loss?
GLP-1 receptor agonists like Semaglutide (Ozempic) and Tirzepatide (Mounjaro) cause the most significant weight loss among all diabetes medications.
Q4. Is insulin the last stage of diabetes?
No. Insulin is not a last stage or punishment. Many doctors now start insulin earlier to protect organs from damage. Starting insulin when needed is a sign of good medical care — not disease worsening.
Q5. What are the 5 antidiabetic drug?
The 5 main classes of antidiabetic drugs are:
Metformin (Biguanides) — first-line treatment
Sulfonylureas (Glimepiride, Gliclazide) — stimulate insulin release
SGLT2 Inhibitors (Jardiance, Forxiga) — flush sugar through urine
GLP-1 Agonists (Ozempic, Trulicity) — gut hormone mimics
DPP-4 Inhibitors (Januvia, Galvus) — protect natural gut hormones
Your doctor selects the right combination based on your HbA1c, weight, kidney function and budget.
Q6. What happens if I skip my diabetes medicine?
Skipping diabetes medicine — even for one day — can cause blood sugar to rise significantly. Over time, consistently skipping medication leads to:
HbA1c rising above target
Silent damage to kidneys, eyes and nerves
Higher risk of heart attack and stroke
Faster progression to needing insulin
Never skip medication without consulting your doctor.
Reference
H2 1 — Why Medication is Needed Alongside Lifestyle Changes
- ADA + AACE Pharmacologic Recommendations 2024 — University of Illinois Chicago Drug Information Group
- Common Crossroads in Diabetes Management — PMC
- ADA Standards of Care in Diabetes 2024 — American Diabetes Association
H2 2 — Metformin
- Metformin — StatPearls, NIH Bookshelf
- Metformin: Update on Mechanisms of Action — Nature Reviews Endocrinology 2023
- Understanding Metformin Action in the GI Tract — Frontiers in Pharmacology 2024
- Metformin: Diverse Molecular Mechanisms — PMC 2024
H2 3 — GLP-1 Receptor Agonists
- GLP-1 Single, Dual and Triple Receptor Agonists — The Lancet eClinicalMedicine 2024
- GLP-1 Receptor Agonists in Type 2 Diabetes — State of the Art — PMC
- Emerging Frontiers in GLP-1 Therapeutics 2025 — PMC
- Safety and Efficacy of GLP-1 Receptor Agonists — PMC 2024
H2 4 — SGLT2 Inhibitors
- Protective Influence of SGLT-2 Inhibitors Against Heart Failure — PMC 2024
- Clinical Evidence for Cardiovascular and Kidney Benefits of SGLT2 Inhibitors — PMC
- SGLT2 Inhibitors: Antidiabetic and Cardioprotective Effects — PMC
- Emerging Horizons: SGLT-2 Inhibitors Beyond Diabetes — PMC
H2 5 — DPP-4 Inhibitors, Sulfonylureas, TZDs
- ADA + AACE Pharmacologic Recommendations 2024 — UIC Drug Information
- 2024 ADA Standards of Care Update — Endocrinology Advisor
- Metformin StatPearls — Combination Therapy Hierarchy — NIH
H2 6 — Tirzepatide / Mounjaro 2025
- Tirzepatide’s Therapeutic Spectrum: Dual GIP/GLP-1 Agonist — PMC 2025
- Real-World Tirzepatide vs Semaglutide on HbA1c and Weight — PMC 2025
- Tirzepatide Improves Beta-Cell Function and Insulin Sensitivity — PMC
- Efficacy and Safety of Tirzepatide: Systematic Review and Meta-Analysis — PMC
H2 7 — Insulin Types
- Insulin Therapy for Type 2 Diabetes: Rescue, Augmentation and Replacement — AAFP
- The Modern Role of Basal Insulin in Type 2 Diabetes — ADA Diabetes Care 2025
- Diabetes Insulin Therapy — MedlinePlus Medical Encyclopedia
- Bolus Insulin Prescribing Recommendations for T2D — PMC
About the author
It’s me Mohammad Junaid Rain an MBBS student at GMC Nagpur, passionate about making evidence-based medical information accessible to every Indian. “medstuffs.com” is dedicated to clear, doctor-written disease education for patients and caregivers.
Disclaimer: This article is for educational purposes only and does not substitute professional medical advice. Please consult your doctor for diagnosis and treatment.
1 thought on “Type 2 Diabetes Medications: Critical Facts About Metformin, GLP-1 & SGLT2 Every Patient Must Know”