
So before talking about “what is type 2 diabetes”? Let me introduce you with some facts. Right now, over 589 million people worldwide are living with diabetes — and more than 9 out of 10 of them have type 2 diabetes. In the United States alone, that number is close to 40 million people and 101 million in India. The shocking part? Nearly half of them had no idea anything was wrong until their doctor ran a routine blood test.
So — what is type 2 diabetes, exactly? And why should you care right now, today?
Type 2 diabetes is a long-term health condition where your body either stops producing enough insulin or stops responding to insulin the way it should — causing blood sugar levels to rise higher than normal. Unlike type 1 diabetes, type 2 usually develops slowly over time and is closely linked to lifestyle, diet, and family history.
The numbers tell a serious story. According to the International Diabetes Federation (IDF) 2024 Atlas:
589 M
dults worldwide living with diabetes
101 M
people with diabetes in India
40 M
Americans currently diagnosed
>90%
Among all diabetes more than 90% are type 2
These aren’t just numbers on a page — this is a condition that affects real families, real daily routines, and real quality of life. And the earlier you understand it, the better your chances of managing or even preventing it. Let me guide you to understand about “what is type 2 diabetes”?
This guide breaks down everything you need to know about type 2 diabetes in simple, everyday language — no medical degree required.
Whether you’ve just been diagnosed with type 2 diabetes, you’re concerned about your blood sugar levels, caring for a family member, or simply want to understand what prediabetes really means — this guide is written for you. No medical background needed. Just clear, honest information you can actually use.
What is type 2 diabetes? (And how is it different from type 1?)
Diabetes, at its core, is a blood sugar problem
To understand what is type 2 diabetes, you first need to understand one simple thing: what blood sugar actually does in your body.
Every time you eat — a bowl of rice, a piece of bread, even a banana — your body breaks that food down into glucose (sugar). That glucose enters your bloodstream and needs to get inside your cells to give you energy. Think of glucose as the fuel, and your cells as the engine.
But here’s the catch: glucose can’t just walk into your cells on its own. It needs a key. That key is a hormone called insulin, made by your pancreas. When insulin bind to the cell it will open the door for the entry of glucose in the cells.
Imagine insulin as a doorman standing outside every cell in your body. When glucose shows up, insulin opens the door and lets it in. In type 2 diabetes, either the doorman stops showing up which is obviously insulin — or the doors stop responding to him altogether.
When this system breaks down, glucose piles up in your bloodstream instead of entering your cells. Over time, that excess blood sugar starts damaging your blood vessels, nerves, kidneys, and eyes — often without any obvious warning signs for years.
Type 1 vs type 2 diabetes — what’s the difference?
| Feature | Type 1 diabetes | Type 2 diabetes |
|---|---|---|
| What goes wrong | Immune system destroys insulin-making cells | Body stops responding to insulin properly |
| Insulin production | Little to none | Present, but ineffective or declining |
| Who gets it | Usually children and young adults | Mostly adults 40+, but rising in youth |
| Onset speed | Sudden (days to weeks) | Gradual (years, often silent) |
| Share of cases | ~5–10% | >90% of all diabetes |
| Can lifestyle help? | No — requires insulin therapy | Yes — diet, exercise, and weight loss can help significantly |
| Preventable? | No | Often yes, especially if caught early |
How prediabetes quietly becomes type 2 diabetes
Type 2 diabetes rarely appears overnight. It usually follows a slow, silent path — and there’s a crucial stage in between called prediabetes.
During the prediabetes stage, your blood sugar is higher than normal — but not yet high enough for a full type 2 diabetes diagnosis. This is the window where lifestyle changes can actually reverse the direction. Many people in this stage have no symptoms at all, which is why regular blood sugar testing matters so much.
In India alone, over 136 million people currently have prediabetes. In the US, that number is 97.6 million — nearly 1 in 3 adults. Most of them don’t know it yet.
The real reason type 2 diabetes develops: two things go wrong at once
At the heart of type 2 diabetes is a two-part failure. Understanding this helps everything else make sense.
Insulin resistance
Your muscle, fat, and liver cells stop responding to insulin’s signal. The “key” is there, but the “locks” on the cell doors are broken. Your pancreas compensates by pumping out more and more insulin — until it can’t keep up.
Beta cell failure
Beta cells are the tiny cells in your pancreas that make insulin. In type 2 diabetes, years of overwork wear them down. Over time, they produce less and less insulin — making blood sugar control even harder.
Together, these two problems — insulin resistance and beta cell failure — are what define type 2 diabetes. One makes your body ignore insulin. The other makes your body produce less insulin. The result is blood sugar levels that stay dangerously high, quietly causing damage throughout your body.
Type 2 diabetes = insulin resistance + beta cell failure.
How does type 2 diabetes develop?
The 5-step breakdown: how type 2 diabetes takes hold.
1. Insulin resistance begins in muscle and fat cells
It usually starts silently, years before any diagnosis. Your muscle cells — which normally absorb most of the glucose in your blood — begin ignoring insulin’s signal. Fat cells follow. The “doors” to your cells stop responding to insulin’s key. Blood sugar starts rising after meals, but your pancreas compensates by producing more insulin. At this stage, most people feel completely normal. But the problem towards type 2 diabetes has already begins.
2. The pancreas overworks — and beta cells begin to burn out
To keep blood sugar in check, your pancreas produces high amounts of insulin. The beta cells — tiny insulin factories inside the pancreas — are working overtime. Over months and years, this relentless demand wears them down. Beta cell mass literally shrinks. At some point, the pancreas simply can’t keep up, and blood sugar starts staying high even between meals.
3. The liver adds fuel to the fire
Normally, insulin tells your liver to stop releasing glucose into the blood when sugar levels are already high. But in insulin resistance, the liver ignores this signal too — and keeps pouring glucose into the bloodstream even when it’s not needed. This is called hepatic glucose overproduction, and it’s a major reason blood sugar stays elevated overnight and first thing in the morning — even without eating.
4. Glucagon goes abnormal
Glucagon is insulin’s opposite — a hormone that raises blood sugar when it drops too low. In a healthy body, insulin and glucagon balance each other. In type 2 diabetes, glucagon levels stay abnormally high, even after meals. Instead of dropping when blood sugar rises, glucagon keeps stimulating the liver to release more glucose. It’s like pressing the accelerator and the brake at the same time — the system loses control.
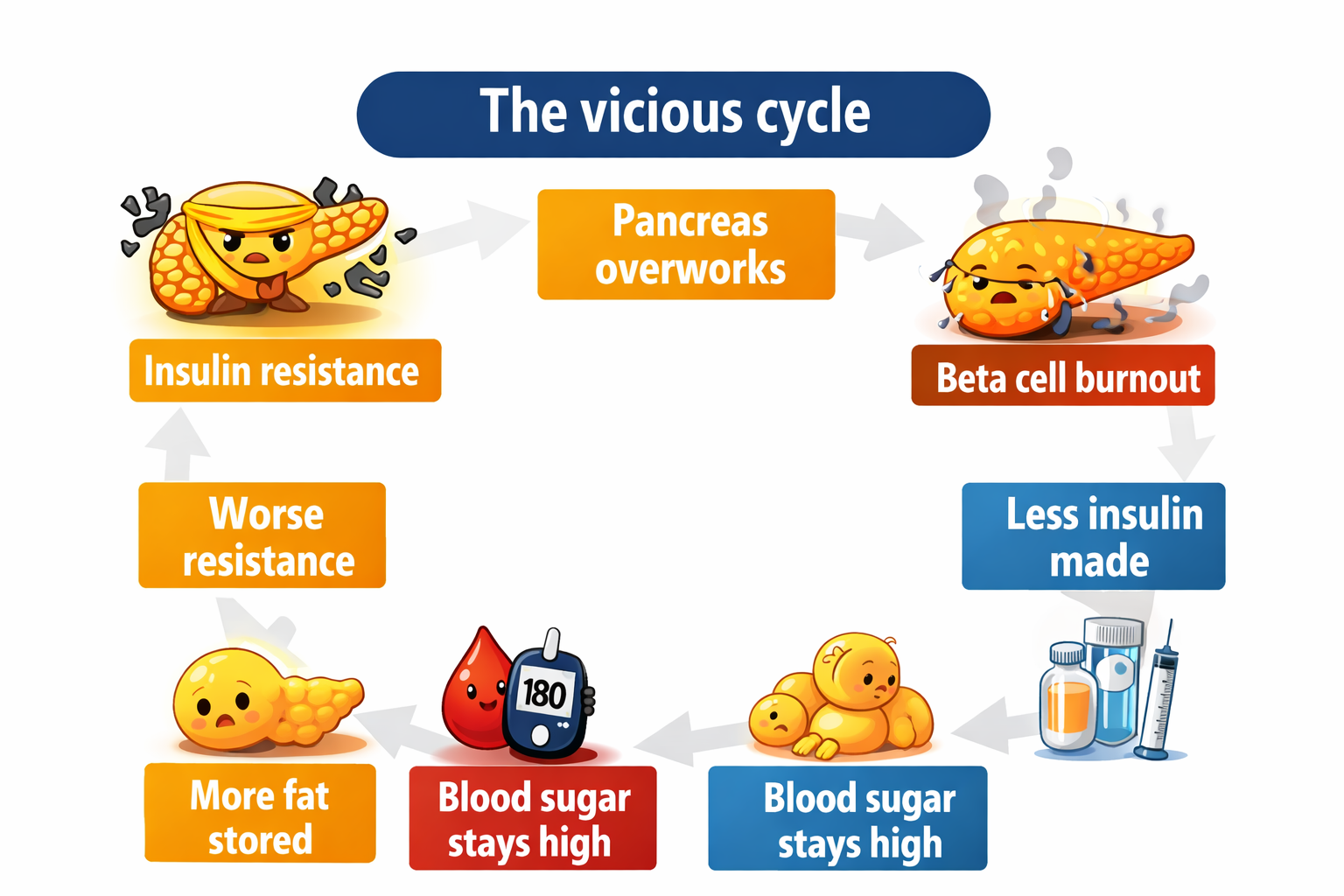
5. fat cells triggers chronic inflammation
Excess fat — especially visceral fat deep around your organs — doesn’t just sit there. It actively secretes inflammatory molecules called cytokines. These chemicals interfere with insulin signalling across the whole body, worsening insulin resistance further. This creates a vicious cycle: more fat leads to more inflammation, which leads to worse insulin resistance, which makes blood sugar harder to control, which leads to more fat storage.
What goes wrong and where?
Pancreas
Normally: makes insulin on demand
In Type-2-D: beta cells burn out, less insulin made
Muscle cells
Normally: absorb glucose with insulin’s help
In T2D: resist insulin signal, glucose stays in blood
Liver
Normally: stops releasing glucose when insulin rises
In T2D: keeps releasing glucose — even after meals
Fat cells
Normally: store energy, minimal signalling
In T2D: release inflammatory molecules, worsen resistance
Glucagon
Normally: rises only when blood sugar is low
In T2D: stays high — pushes blood sugar up constantly
1) Pancreas
Beta cells burn out, less insulin produced.
2) Muscles
Cells resist insulin, glucose can’t enter
3) Liver
Keeps dumping glucose even after meals
4) Fat cells
Inflame the body, worsen resistance
6) Glucagon
Stuck in “raise blood sugar” mode constantly
Why does this matter for you? Each of these five failure points is actually a treatment target. Modern type 2 diabetes medications — like metformin, GLP-1 agonists, and SGLT2 inhibitors — work by fixing different parts of this broken system. Understanding the “why” makes treatment make sense. We’ll cover that in full in the treatment section.
So what does all this actually feel like? The tricky part about type 2 diabetes is that this entire breakdown can unfold over 5–10 years with almost no obvious symptoms. In the next section, we cover the early warning signs your body sends — and why so many people miss them until it’s too late.
Who is at risk for type 2 diabetes? 7 key risk factors explained
One of the most important things to understand about what is type 2 diabetes is this: it doesn’t pick people at random. There are clear, well-documented risk factors that significantly raise your chances of developing it — and knowing them could genuinely change what you do next.
Some of these you can’t control. Others you absolutely can. Here’s what the latest research, including the American Diabetes Association (ADA) 2025 Standards of Care, says about who is most at risk.
Age (45+)
Risk rises significantly after age 45. Cells become less sensitive to insulin as we age, and the pancreas naturally becomes less efficient over time.
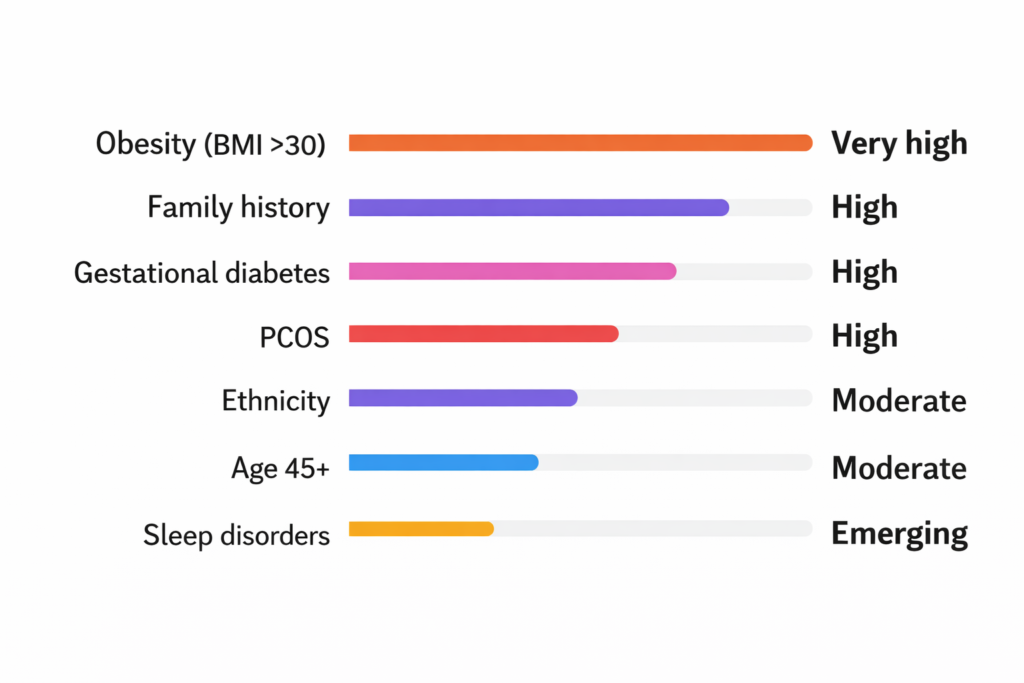
Obesity/high BMI
Excess body fat — especially around the belly — is the single biggest modifiable risk factor. Fat cells interfere directly with how insulin works.
BMI >30 Higher risk
Ethnicity disparities
South Asians (including Indians), Black, Hispanic, and Indigenous populations face significantly higher risk — often at lower BMI levels than white populations.
South Asians risk of type-2-D is at lower BMI also.
Family history
If a parent or sibling has type 2 diabetes, your risk is 2–3× higher. Genetics influence how your cells respond to insulin and how your pancreas functions.
Gestational diabetes
Women who developed diabetes during pregnancy have up to a 50% lifetime risk of developing type 2 diabetes within 5–10 years after delivery.
upto 50% risk lifetime
Sleep disorders
The ADA’s 2025 guidelines now formally recognize poor sleep and sleep apnea as independent risk factors. Disrupted sleep raises cortisol and directly impairs insulin sensitivity.
PCOS
Women with polycystic ovary syndrome (PCOS) have significantly elevated insulin resistance, making them one of the highest-risk groups for developing type 2 diabetes.
These females have higher risk of type-2-D than avg female.
How compare these risk factors?
For the first time, the American Diabetes Association’s Standards of Care officially lists sleep health as a diabetes risk factor. If you regularly sleep fewer than 6 hours a night or have been told you snore heavily, it’s worth bringing up with your doctor — not just for sleep, but for your blood sugar too.
A note for South Asian readers (including India)
If you’re from South Asia — India, Pakistan, Bangladesh, Sri Lanka — your risk profile is uniquely different from Western populations. Research shows that type 2 diabetes develops in South Asians at a lower BMI, younger age, and with less obvious obesity compared to white European populations.
This means standard BMI cutoffs (like 25 or 30) may not apply to you the same way. Indian health guidelines recommend screening for diabetes starting at a BMI of 23 — and from age 35 onwards, rather than 45.
Do you have one or more of these risk factors?Having a risk factor doesn’t mean you will develop type 2 diabetes — but it does mean your body may already be giving you warning signs. In the next section, we cover the early symptoms of type 2 diabetes that most people miss for years.
Signs and symptoms of type 2 diabetes
Here’s what makes type 2 diabetes so dangerous: it is almost completely silent in the early stages. Most people live with high blood sugar for 5 to 10 years before getting a diagnosis — not because they ignored it, but because their body gave them almost no obvious warning.
But when symptoms do appear, they follow a recognisable pattern. Knowing what to look for could save your life — or someone else’s.
The classic trio — the three most recognised symptoms
Doctors have a name for the three hallmark symptoms of diabetes. They all start with “poly” — which simply means “too much.”
- Polyuria -Urinating far more than usual, especially at night.
- Polydipsia – Extreme, unquenchable thirst — even after drinking.
- Polyphagia – Constant hunger, even shortly after eating a full meal.
These three symptoms happen because high blood sugar overwhelms the kidneys, which start flushing excess glucose out through urine — taking large amounts of water with it. That causes dehydration (thirst), fluid loss (frequent urination), and because glucose can’t enter the cells for energy, your body keeps signalling hunger.
All the symptoms — from common to easy to miss
Frequent urination
Needing to urinate often — including waking up multiple times at night. Kidneys are working overtime to flush out excess blood sugar.
Extreme thirst
Constant thirst that doesn’t go away no matter how much you drink. Your body is losing fluids fast through all that extra urination.
Constant hunger
Always feeling hungry, even after meals. Your cells aren’t getting the glucose they need for energy — so your brain keeps asking for more food.
Unexplained fatigue
Feeling deeply tired even after a full night’s sleep. Without glucose getting inside cells, your body is running on empty — no matter how much you eat or rest.
Blurred vision
High blood sugar pulls fluid from the lenses of your eyes, changing their shape and blurring your focus. Many people blame their glasses prescription — not their blood sugar.
Slow-healing wounds
A cut or sore that takes weeks to heal — or won’t heal at all — is a serious red flag. High blood sugar damages blood vessels and nerves, reducing blood flow and immune response to injuries.
Tingling/ numb feets
Tingling, numbness, or a burning sensation in the feet or hands is a sign of diabetic neuropathy — nerve damage from prolonged high blood sugar. This can appear even before a formal diagnosis.
Recurring infections
Frequent yeast infections, urinary tract infections, or skin infections that keep coming back. High glucose is essentially food for bacteria and fungi — making infections harder to fight off.
The silent years — why most people don’t know they have it
Important: Type 2 diabetes can be completely silent for years. Many people are only diagnosed during a routine blood test — not because they felt sick. This is why screening matters just as much as symptoms.
Years 1–3: Insulin resistance building quietly. Blood sugar slightly elevated after meals. No noticeable symptoms. Most people feel completely normal.
Years 3–6: Fatigue, occasional thirst, and blurred vision may appear — but are often blamed on stress, ageing, or dehydration. Still frequently undiagnosed.
Years 6–9: Classic symptoms become more persistent. Slow-healing wounds, tingling feet, and frequent infections may appear. Many are diagnosed at this stage — often by accident.
Year 10+: If still undiagnosed or unmanaged — complications including kidney disease, vision loss, and cardiovascular damage may begin. This is entirely preventable with early detection.
When should you see a doctor?
Not every symptom means you have type 2 diabetes — but some combinations are worth acting on promptly. Here’s a simple guide:
Book a routine checkup: If you have 1–2 risk factors and mild fatigue or thirst.
See your doctor soon: If you have multiple symptoms lasting more than 2–3 weeks.
See a doctor now: Wound not healing, sudden vision loss, or numbness spreading.
Tell your doctor if you have seen any of these combinations:
- Unusual thirst + frequent urination + unexplained fatigue — even if mild
- A cut, sore, or wound that hasn’t healed in 2+ weeks
- Tingling, burning, or numbness in your feet or hands
- Blurred vision that comes and goes with no clear reason
- Recurring thrush, UTIs, or skin infections with no obvious cause
- You have risk factors (age 45+, family history, high BMI) and haven’t been tested in over a year
Suspect you might have type 2 diabetes? The next step is a blood test. In the next section, we break down exactly how type 2 diabetes is diagnosed — including the HbA1c test, fasting glucose, and what your numbers actually mean
How is type 2 diabetes diagnosed? The 4 tests and what your numbers mean
Getting diagnosed with type 2 diabetes comes down to one thing: a blood test. There’s no guesswork involved — it’s measured, objective, and confirmed with numbers. The tricky part is understanding what those numbers actually tells
There are four tests your doctor may use. Each measures blood sugar differently — and each has a specific cutoff that separates normal, prediabetes, and diabetes.
These tests are like speed cameras on a road. One catches your average speed over months (HbA1c). One catches you right now, with no preparation (random glucose). One catches you after an overnight fast (fasting glucose). And one watches how you handle a sugar load (OGTT). Together, they give doctors a complete picture.
The 4 blood tests used to diagnose type 2 diabetes:
HbA1C
3-month average
≥ 6.5%
Measures the percentage of haemoglobin coated with sugar over the past 2–3 months. No fasting required. A single result can confirm diagnosis if symptoms are present.
Fasting blood glucose
After 8hr fast
≥ 126 mg/dL
Blood sugar measured after at least 8 hours without eating. Taken first thing in the morning. One of the most commonly used tests at routine health check-ups.
Random plasma glucose
Any time of day
≥ 200 mg/dL
A blood sugar test taken at any time, regardless of when you last ate. Only used for diagnosis when classic symptoms (thirst, urination, fatigue) are clearly present.
OGTT
2hr after glucose drink
≥ 200 mg/dL
Oral glucose tolerance test — you drink a sugary solution and blood sugar is measured 2 hours later. Most thorough test, used in pregnancy screening and borderline cases.
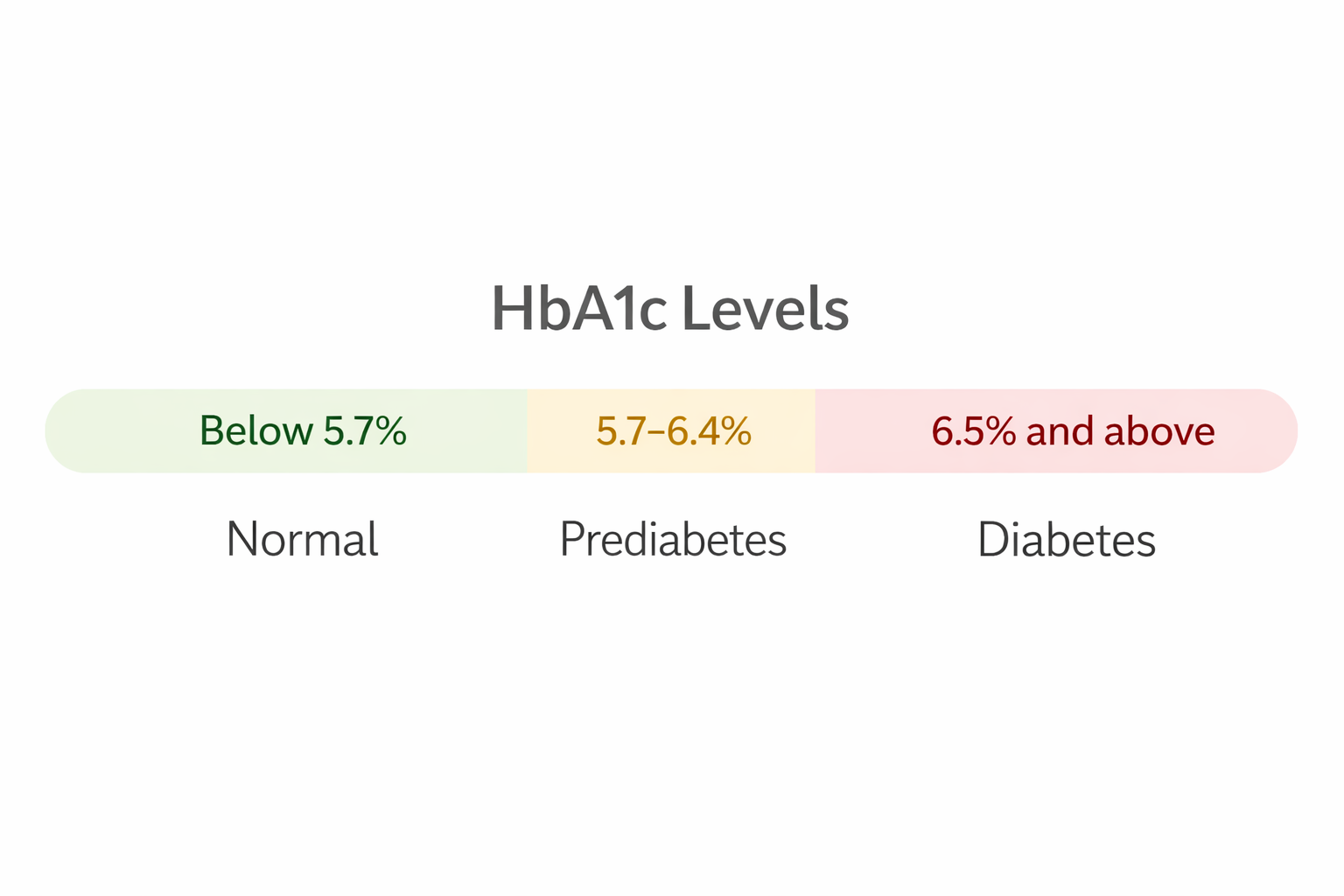
Understanding your HbA1c number
The HbA1c test is the most widely used because it doesn’t require fasting and reflects your average blood sugar over the past 2–3 months — not just one moment in time. Here’s what the range looks like:
Every 1% rise in HbA1c above 6.5% roughly corresponds to a meaningful increase in the risk of complications — especially for your kidneys, eyes, and nerves. This is why getting to your target HbA1c matters so much after diagnosis.
Diagnostic criteria table — ADA 2026 standards
This is the official reference table your doctor uses. These are the thresholds that define normal blood sugar, prediabetes, and type 2 diabetes according to the American Diabetes Association 2026 Standards of Care:
| Test | Normal | Prediabetes | Diabetes |
| HbA1c | Below 5.7% | 5.7–6.4% | >= 6.5% |
| Fasting glucose | < 100 mg/dL | 100–125 mg/dL | ≥ 126 mg/dL |
| OGTT (2-hour) | < 140 mg/dL | 140–199 mg/dL | ≥ 200 mg/dL |
| Random glucose | — | — | >= 200 mg/dl + symptoms |
Important — confirmation rule: A single abnormal result is usually confirmed with a second test on a different day — unless you have clear symptoms and a random glucose of ≥ 200 mg/dL, or two different abnormal tests are done at the same visit. One test is rarely enough for a final diagnosis on its own.
Who should get screened — and how often?
You don’t need symptoms to get tested. The ADA recommends routine screening for type 2 diabetes based on age and risk profile — because catching it early, or at the prediabetes stage, dramatically changes outcomes.
All adults age 35+
Routine screening regardless of symptoms or risk factors
Every 3 years if normal
Overweight adults
BMI ≥25 (or ≥23 for South Asians) with one or more risk factors
Every 1–2 years
Gestational diabetes history
Post-pregnancy screening at 6–12 weeks, then ongoing
Every 1–3 years
Prediabetes diagnosed
Already in the at-risk zone — active monitoring needed
Every year
For children/teens
If overweight + family history or other risk factors
From age 10 onwards
HIV-positive adults
ADA 2026 now includes HIV as an independent screening trigger
Every 1–2 year
For Indian readers: Indian guidelines (RSSDI / ICMR) recommend starting screening from age 30 — not 35 — given that South Asians develop type 2 diabetes earlier and at lower BMI. If you’re over 30 with any risk factor, ask your doctor for an HbA1c or fasting glucose test at your next visit.
Got your results — and wondering what to do next? A diagnosis of type 2 diabetes isn’t the end of the story. In the next section, we break down exactly how type 2 diabetes is treated — from first-line lifestyle changes to medications like metformin, GLP-1 agonists, and what the latest 2026 guidelines recommend.
Managing type 2 diabetes: lifestyle changes that actually work
Here’s something most people aren’t told at diagnosis: type 2 diabetes is one of the few chronic conditions where lifestyle changes can be as powerful — sometimes more powerful — than medication. In some cases, they can push the condition into full remission.
This isn’t wishful thinking. It’s what the latest clinical evidence, including the ADA 2025 Standards of Care, consistently shows. Here’s what works, and by how much.
1) 0.6–1% HbA1c drop from diet alone.
2) 0.5–0.7% HbA1c drop from exercise alone.
3) 5–10% Weight loss needed to see significant improvement.
4) 50% Reduced risk of progression from prediabetes with lifestyle.
Best diet for type 2 diabetes
1) Mediterranean diet
Rich in vegetables, legumes, whole grains, olive oil, fish, and nuts. Low in red meat and processed foods. Reduces HbA1c and cardiovascular risk simultaneously — the two biggest concerns in type 2 diabetes.
HbA1c reduction: 0.3–0.5%
2) Low carbohydrate diet
Restricting carbohydrates to under 130g/day directly reduces blood sugar spikes after meals. Studies show it lowers HbA1c faster than low-fat diets in the short term — especially effective in the first 3–6 months.
HbA1c reduction: up to 0.9%
3) Plate method
Half your plate: non-starchy vegetables. A quarter: lean protein. A quarter: complex carbs. No calorie counting required — just a visual framework that naturally controls portions and blood sugar. Recommended as a starting point by the ADA.
Eat more of these
- Leafy greens and non-starchy vegetables
- Whole grains (oats, brown rice, millets)
- Legumes (dal, rajma, chana)
- Fatty fish (salmon, sardines)
- Nuts and seeds
- Olive oil and healthy fats
Eat less of these
- White rice, white bread, maida
- Sugary drinks and fruit juices
- Ultra-processed snacks and biscuits
- Fried foods and trans fats
- Red and processed meats
- Full-fat dairy in large amounts
Weight loss — even a small amount makes a big difference
You don’t need to reach your “ideal” weight to see meaningful improvements in blood sugar. Research — including the landmark DiRECT trial — shows that even modest weight loss produces significant, measurable results.
The DiRECT Trial finding: In a landmark UK study, nearly half of participants who lost 15kg or more achieved full remission of type 2 diabetes — with normal blood sugar and no medication — after one year. Weight loss is not just “helpful.” For many people, it is the most powerful intervention available.
Physical activity — the free medication most people underuse
Exercise works like a second key for your cells. When you move your muscles, they absorb glucose directly — without needing insulin. This is why even a 15-minute walk after a meal can noticeably lower your post-meal blood sugar.
The ADA recommends a specific combination of activity types for people with type 2 diabetes:
Aerobic exercise
150 min/week
Walking, cycling, swimming, dancing. Spread across at least 3 days. Directly lowers blood sugar and improves insulin sensitivity.
Strength training
(2–3)× / week
Resistance bands, weights, or bodyweight exercises. Builds muscle mass — and muscle is your body’s biggest glucose absorber.
Break sitting time
Every 30 minute
New ADA 2025 guidance: prolonged sitting independently raises blood sugar. Stand up, walk for 3 minutes every half hour if you have a desk job.
Daily steps
7000-10,000
If structured exercise feels overwhelming, just walking more is a strong starting point. Step count is one of the best-studied and most accessible activity targets.
Sleep — the metabolic lever most people ignore ADA 2025
Sleep is no longer just a wellness tip. The ADA’s 2025 Standards of Care formally recognised poor sleep as an independent factor that worsens blood sugar control — and improving it as a legitimate management strategy.
What poor sleep does to blood sugar?
Even a single night of poor sleep raises cortisol and growth hormone — both of which increase insulin resistance the following day. Chronic sleep deprivation (under 6 hours) raises HbA1c independently of diet or exercise. Treating sleep apnoea in people with type 2 diabetes has been shown to lower HbA1c by 0.3–0.5% on its own. The ADA now recommends screening all people with type 2 diabetes for sleep disorders — not just as a side issue, but as part of standard metabolic care.
The other lifestyle levers — stress, alcohol, and smoking
- stress management – Chronic stress raises cortisol, which directly raises blood sugar — even without eating. Mindfulness, yoga, and structured breathing have clinical evidence behind them in diabetes management. Even 10 minutes a day of relaxation practice measurably affects cortisol levels.
- Alcohol – Alcohol causes unpredictable swings in blood sugar — it can raise it sharply immediately, then cause a dangerous drop hours later. If you drink, the ADA recommends no more than 1 unit/day for women and 2 for men, always with food, and never on an empty stomach. (disclaimer – it is advised not to drink alcohol)
- Smoking – Smoking dramatically worsens insulin resistance and increases the risk of every diabetes complication — heart disease, kidney failure, nerve damage, and amputation. Quitting smoking is one of the single most impactful things a person with type 2 diabetes can do.
Lifestyle changes are the foundation — but sometimes medication is needed too. In the next section, we cover the full range of type 2 diabetes medications — from metformin to GLP-1 receptor agonists — what they do, who they’re for, and what the latest ADA 2026 guidelines recommend as first-line treatment.
Type 2 diabetes medications — what they are, how they work, and who they’re for
Lifestyle changes are the foundation of type 2 diabetes management — but for most people, medication is also needed, at least initially. The good news is that the treatment toolkit has never been better. Today’s medications don’t just lower blood sugar — many of them protect your heart, kidneys, and help with weight loss at the same time.
The full medication toolkit — 6 drug classes explained
- Metformin– Reduces glucose production in the liver. Improves insulin sensitivity in muscle cells. Taken orally, usually twice daily with meals.
- GLP-1-agonist- Mimic a gut hormone that boosts insulin after meals, suppresses glucagon, and slows digestion. Also signals the brain to reduce appetite — making these the most powerful weight-loss drugs in diabetes care.
- SGLT-2 inhibitors- Force the kidneys to excrete excess glucose in the urine — literally flushing sugar out of the body. Also lower blood pressure, reduce heart failure risk, and slow kidney disease progression.
- DPP-4 inhibitors- Block the enzyme that breaks down GLP-1 in the body — indirectly boosting insulin response after meals. Gentler effect than GLP-1 injections. Taken as a daily oral tablet. Well tolerated, minimal side effects.
- Dual GLP-1/GIP agonist- The newest class — activates two gut hormone receptors simultaneously (GLP-1 and GIP). Produces the greatest HbA1c reduction and weight loss of any diabetes drug currently available. ADA 2026 now recommends it as a preferred option when weight loss is a priority.
- Insulin therapy- It is used when other medications aren’t sufficient to control blood sugar. Not a sign of failure — simply the next step. Modern long-acting insulins are taken once daily and cause far less hypoglycaemia than older formulations.
GLP-1 agonists in focus — Ozempic, Trulicity, and Mounjaro
GLP-1 receptor agonists are the most talked-about class in diabetes care right now — and for good reason. They lower blood sugar, promote significant weight loss, and protect the heart and kidneys. Here’s how the main options compare:
Semaglutide
Ozempic (weekly injection) / Rybelsus (oral)
HbA1c reduction: ~1.5%. Weight loss: 5–10%. Strong cardiovascular evidence.
Dulaglutide
Trulicity (weekly injection)
HbA1c reduction: ~1.2%. Weight loss: 3–5%. Well tolerated, proven heart benefit.
Tirzepatide
Mounjaro (weekly injection)
HbA1c reduction: up to 2.4%. Weight loss: 15–20%. Dual GLP-1/GIP action. Preferred by ADA 2026 when weight loss is a priority.
Liraglutide
Victoza (daily injection)
HbA1c reduction: ~1.0–1.5%. Weight loss: 3–4%. Longest cardiovascular safety data.
How treatment is stepped up — the ADA 2026 approach
Treatment for type 2 diabetes isn’t one-size-fits-all. The ADA 2026 guidelines recommend a personalised, stepwise approach based on your HbA1c, weight, kidney function, and heart health:
1. Lifestyle changes alone
For newly diagnosed patients with HbA1c close to target (under 7.5%). Diet, exercise, weight loss, and sleep improvement attempted first for 3 months.At diagnosis — if HbA1c < 7.5%
2. Metformin + lifestyle
Standard first-line combination. Metformin added immediately if HbA1c is above target, or if lifestyle changes alone don’t achieve control within 3 months.Most common starting point
3. Add GLP-1 agonist or SGLT2 inhibitor
If blood sugar isn’t controlled with metformin alone — or if you have heart disease, heart failure, or kidney disease — ADA 2026 recommends adding a GLP-1 agonist or SGLT2 inhibitor regardless of HbA1c level.Heart / kidney disease: add immediately
4. Triple therapy or dual agonist
Combination of two or three drug classes. Mounjaro (tirzepatide) increasingly preferred at this stage when weight loss is a significant goal alongside blood sugar control.
5. Insulin therapy
Added when other combinations are insufficient, or in situations of very high HbA1c at diagnosis (above 10%). Not a last resort — simply the most direct route to glucose control when needed.
Important — insulin is not a failure: Many people fear being put on insulin, as if it means their diabetes has “got worse” or they “didn’t try hard enough.” This is a myth. Needing insulin simply means your beta cells need more support than tablets can provide. Modern long-acting insulins are safe, easy to use, and dramatically improve quality of life when other options aren’t enough.
Quick comparison — all drug classes at a glance:
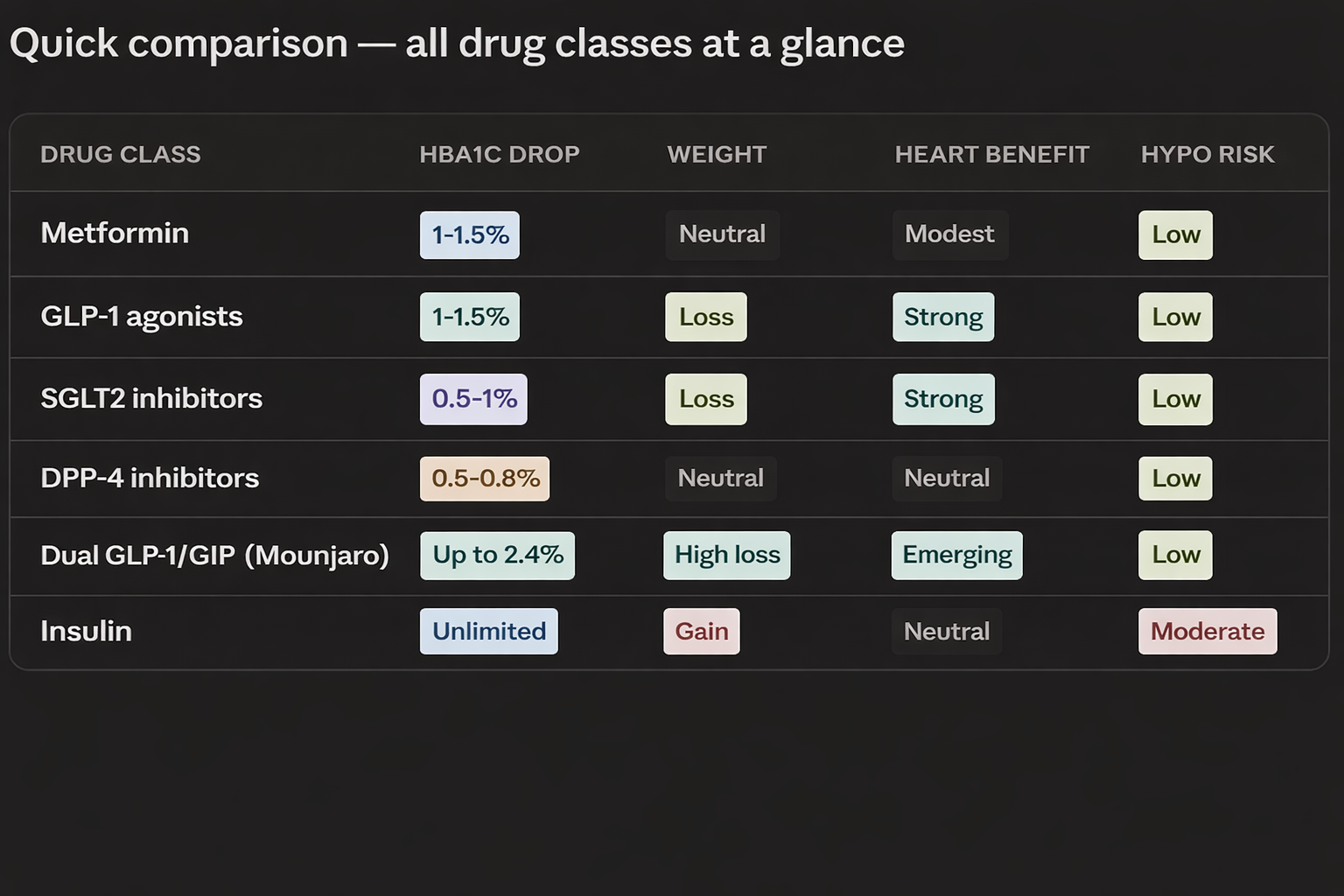
Medical note: Every medication listed here requires a prescription and should only be started, changed, or stopped under the guidance of your doctor. The right medication for you depends on your HbA1c, kidney function, heart health, weight goals, and personal preference. This section is for information only — not a substitute for medical advice.
Medications manage blood sugar — but what about complications?Even well-controlled type 2 diabetes can lead to serious complications over time if not monitored properly. In the next section, we cover diabetic complications — from neuropathy to retinopathy — what causes them, how to detect them early, and how to prevent them.
Complications of type 2 diabetes — what can go wrong, and how to prevent it
Uncontrolled type 2 diabetes doesn’t just affect your blood sugar. Over time, high glucose damages blood vessels and nerves throughout the entire body. These are called diabetic complications — and most of them are preventable with early, consistent management.
Complications develop slowly and silently. Most people don’t notice the damage until it’s advanced. Regular check-ups, blood tests, and eye and foot exams exist specifically to catch problems before they become serious.
People with type 2 diabetes are 2–4 times more likely to have a heart attack or stroke. High blood sugar damages artery walls over time, causing them to narrow and harden. This is the leading cause of death in people with diabetes — which is why GLP-1 and SGLT2 drugs that protect the heart are now prioritised in treatment.Leading cause of death in T2D
2. Diabetic kidney disease (CKD)
High blood sugar gradually damages the tiny filters in the kidneys. Over time this leads to chronic kidney disease — and in severe cases, dialysis. About 1 in 3 people with diabetes develop kidney disease. Early detection through a simple urine test (checking for albumin) can catch it years before symptoms appear.1 in 3 people with T2D affected
3. Neuropathy — nerve damage
Tingling, numbness, or burning pain — usually starting in the feet and moving upward. This is diabetic neuropathy, caused by years of high blood sugar damaging nerve fibres. It affects up to 50% of people with long-standing diabetes. There’s no cure, but good blood sugar control slows it down significantly.Affects up to 50% of long-term T2D
4. Foot complications
A combination of nerve damage and poor circulation means cuts and sores on the feet heal very slowly — or not at all. Infections can develop quickly. In severe cases, this leads to amputation. Simple daily foot checks and proper footwear can prevent most serious foot complications from ever developing. Check your feet every day
5. Retinopathy — eye damage
High blood sugar damages the tiny blood vessels inside the retina. This is called diabetic retinopathy — the leading cause of blindness in working-age adults. It has no symptoms until it’s advanced, which is why an annual dilated eye exam is non-negotiable for anyone with type 2 diabetes.Leading cause of adult blindness
6. Mental health — diabetes distress
Managing a chronic condition every day is exhausting. Diabetes distress — feeling overwhelmed, burned out, or anxious about your condition — affects up to 1 in 3 people with type 2 diabetes. It’s not the same as clinical depression, but it directly worsens blood sugar control. ADA 2026 now recommends annual mental health screening for all people with diabetes.
Most of these complications are preventable — or at least significantly delayed — with good blood sugar control, regular check-ups, and the right medications. Catching them early through routine screening makes all the difference.
Can type 2 diabetes be reversed or put into remission?In the final section, we answer one of the most searched questions about type 2 diabetes — whether it can be reversed — and what the latest evidence from the DiRECT trial and ADA 2026 actually says about remission.
Here is the rewritten section with a warmer, more patient-friendly tone:
Can Type 2 Diabetes Be Reversed?
This is one of the most hopeful questions people ask after being diagnosed with type 2 diabetes — and the good news is: yes, for many people it is absolutely possible. But before we get excited, let’s make sure we understand what “reversed” actually means.
It’s Called Remission — Not a Cure
Doctors prefer the word remission over “reversed” or “cured” — and here’s why that matters.
Remission means your blood sugar returns to a normal, healthy level without needing any diabetes medication. That’s a huge deal. But it doesn’t mean the diabetes has completely disappeared forever. If old habits creep back — weight goes up, diet slips — blood sugar can rise again.
Think of it like this. Remission is like putting out a fire in your kitchen. The fire is gone — but the conditions that caused it are still there. You have to keep managing them. It’s not a cure, but for millions of people, remission means living a completely normal life without medication. That’s worth working towards.
Weight Loss Is the Single Biggest Driver
If there’s one thing the research makes crystal clear, it’s this: losing weight is the most powerful tool for reaching remission.
Here’s why. Extra fat — especially the fat stored deep around your liver and pancreas — is one of the main reasons your body stops responding to insulin properly. When that fat reduces, your insulin starts working better, your pancreas gets some relief, and blood sugar can gradually return to normal.
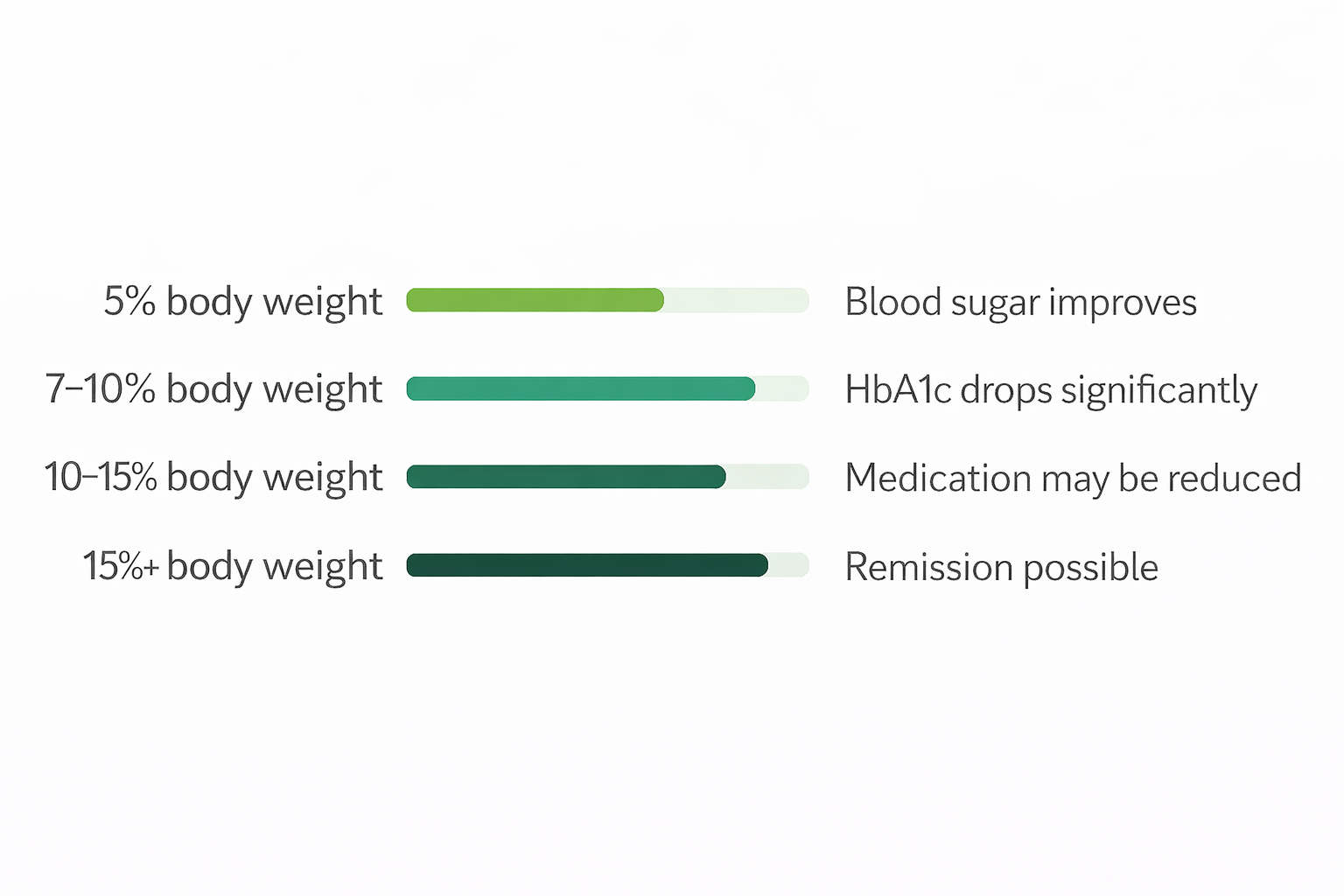
The encouraging part? You don’t need to reach your “ideal” weight to see real results. Research shows that losing just 10 to 15% of your body weight — for example, 8 to 12 kg if you weigh 80 kg — can make a dramatic difference in your blood sugar levels.
The DiRECT Trial — The Study That Changed Everything
If you’ve ever wondered whether remission is really possible, one study answered that question better than any other — the DiRECT trial.
This was a large, well-designed study carried out in the UK. People with type 2 diabetes followed a very low-calorie diet — around 800 calories a day — for 12 to 20 weeks, followed by gradual reintroduction of normal food with ongoing support.
The results were remarkable:
- Nearly 1 in 2 people went into full remission after just one year
- 1 in 3 people were still in remission at two years — off all diabetes medication
- The more weight a person lost, the more likely they were to reach remission
One participant, Kieran, lost 22 kg and has remained in remission for over a decade. His story is not unique — thousands of people have achieved the same.
The message from DiRECT is clear: weight loss isn’t just helpful for diabetes — it can actually reverse it.
What About Bariatric Surgery?
For people who are significantly overweight and haven’t been able to achieve remission through diet alone, bariatric surgery — especially a procedure called gastric bypass — offers some of the highest remission rates of any treatment available.
What’s particularly interesting is that blood sugar often returns to normal within just a few days of surgery — before any major weight loss has even happened. This tells us the surgery also changes important gut hormones that directly improve how the body handles blood sugar.
That said, surgery is a big decision. It carries risks, requires lifelong follow-up, and isn’t the right choice for everyone. It’s a conversation worth having with your doctor if other approaches haven’t worked.
Low-Calorie and Low-Carb Diets — Two Paths That Both Work
The good news is you don’t need surgery to achieve remission. Two dietary approaches have solid scientific evidence behind them:
Very low-calorie diets — cutting down to around 800 calories a day for a set period — produce rapid weight loss and have been shown in studies like DiRECT to push type 2 diabetes into remission. They work fast, but they do require commitment and ideally some medical supervision.
Low-carbohydrate diets — reducing carbohydrates to under 130g per day — work differently. Instead of drastically cutting calories, you reduce the foods that spike blood sugar most directly. This approach lowers blood sugar after meals, improves insulin sensitivity, and is often easier to sustain long term.
FAQ:-
What does type 2 diabetes means?
Type 2 diabetes is a condition where your body either doesn’t make enough insulin or doesn’t use it properly. This causes sugar to build up in your blood instead of going into your cells for energy. It develops slowly over years and is closely linked to weight, diet, and family history.
Is type 2 diabetes curable?
Not cured — but it can go into remission. This means blood sugar returns to normal without medication. Many people achieve this through weight loss, diet changes, or surgery. The more weight you lose, the higher your chances of remission.
What is difference between type 1 and type 2 diabetes?
In type 1, the immune system destroys insulin-making cells. The body makes no insulin at all and always needs insulin injections. It usually starts in childhood and comes on suddenly.
In type 2, the body still makes insulin — but either not enough, or cells stop responding to it. It develops slowly in adults and can often be managed with lifestyle changes and medication.
What are the first warning signs of type 2 diabetes?
The most common early signs are:
Unusual thirst
Frequent urination, especially at night
Unexplained tiredness
Blurred vision
Slow-healing wounds
Tingling or numbness in feet or hands
Many people have no symptoms at all — which is why regular blood tests matter.
Is type 2 diabetes dangerous?
Yes, if left unmanaged. Over time it can lead to heart disease, kidney failure, vision loss, nerve damage, and foot problems. The good news is that most complications are entirely preventable with good blood sugar control and regular check-ups.
How is type 2 diabetes treated?
Treatment is stepwise and personalised:
First — diet, exercise, and weight loss
Second — Metformin (most common first medication)
Third — additional drugs like GLP-1 agonists or SGLT2 inhibitors
Fourth — insulin, if other options aren’t enough
The goal is not just lower blood sugar — it’s protecting your heart, kidneys, and overall health long term.
Common symptoms of type 2 diabetes?
The most common symptoms are extreme thirst, frequent urination, constant tiredness, blurred vision, slow-healing wounds, tingling feet, and recurring infections. Many people have no symptoms at all and are only diagnosed through a routine blood test.
What causes type 2 diabetes?
It’s a combination of factors — excess body weight, physical inactivity, an unhealthy diet, family history, age, and poor sleep. It’s not caused by sugar alone. It develops when your cells stop responding to insulin and your pancreas gradually wears out from overworking.
How is type 2 diabetes diagnosed?
Through a simple blood test. The most common ones are:
HbA1c — no fasting needed, shows 3-month average
Fasting blood sugar — taken after 8 hours without eating
Random blood sugar — taken any time, used when symptoms are present
OGTT — used in pregnancy or borderline cases
A result above the diabetes threshold on two separate tests confirms the diagnosis.
Reference
Standards of Care in Diabetes | ADA Clinical Guidelines
Type 2 Diabetes | Diabetes | CDC
Type 2 Diabetes: What It Is, Causes, Symptoms & Treatment
Global Clinical Practice Recommendations – International Diabetes Federation
Determinants and Stratification of Microvascular Complications of Type 2 Diabetes Mellitus – PMC
About the author
It’s me Mohammad Junaid Rain an MBBS student at GMC Nagpur, passionate about making evidence-based medical information accessible to every Indian. “medstuffs.com” is dedicated to clear, doctor-written disease education for patients and caregivers.
Disclaimer: This article is for educational purposes only and does not substitute professional medical advice. Please consult your doctor for diagnosis and treatment.
13 thoughts on “What Is Type 2 Diabetes? Everything You Need to Know in 2026”