
If you’ve been diagnosed with type 2 diabetes, chances are you were told some version of this:
“It’s a lifelong condition. You’ll need to manage it forever.”
For decades, that was the standard message. But the science has moved on and now we have the answer of the question, can type 2 diabetes be reversed?
Clinical trials and peer-reviewed research now show that type 2 diabetes can go into remission for many people; through specific, evidence-based interventions that target the root cause of the disease.
Remission vs. Reversal vs. Cure
These three words get used interchangeably online. They shouldn’t be. They mean very different things.
Cure means the disease is permanently gone — no monitoring, no risk of return. For type 2 diabetes, no cure exists. Any supplement, program, or clinic claiming otherwise is misleading you.
Reversal is the popular term — used by influencers, wellness blogs, and even some clinicians. The problem is it implies the disease is fully undone, which the evidence doesn’t support. The underlying vulnerability to insulin resistance doesn’t simply disappear. This is why the medical community moved away from this word.
Remission is what the science actually uses — and it’s the most honest term.
In 2021, an expert panel convened by the American Diabetes Association (ADA), alongside the Endocrine Society, EASD, and Diabetes UK, published a formal consensus definition:
Remission = HbA1c below 6.5%, sustained for at least 3 months, without any glucose-lowering medications.
Here’s a simple breakdown:
| Term | What It Means | Accurate for T2D? |
|---|---|---|
| Cure | Permanently gone | Doesn’t exist |
| Reversal | Disease “undone” | Imprecise |
| Remission | Blood sugar normalised, off meds | Medically correct |
Remission is real. It’s achievable for many people. But it requires understanding exactly what you’re working toward — and what it takes to get there.
Source: https://diabetesjournals.org/care/article/44/10/2438/138556
The DiRECT trial — landmark evidence for remission
For years, the idea that type 2 diabetes could go into remission through diet alone was largely dismissed by mainstream medicine. Interesting in theory, but not proven in practice.
Then came the DiRECT trial — and everything changed.
What Was the DiRECT Trial?
DiRECT stands for Diabetes Remission Clinical Trial. It was a rigorously designed, cluster-randomised controlled trial conducted across primary care practices in the UK, led by researchers at the Universities of Glasgow and Newcastle.
The study recruited 306 adults who had been diagnosed with type 2 diabetes within the previous six years. Participants had a BMI between 27 and 45, and none were on insulin.
One group received standard diabetes care — the kind of management most people with type 2 diabetes get from their doctor today. The other group followed a structured, low-calorie weight management programme that began with total meal replacement.
No surgery. No new medications. Just a carefully controlled dietary intervention delivered entirely through primary care.
What Did It Find?
The results, published in The Lancet in 2017, were striking.
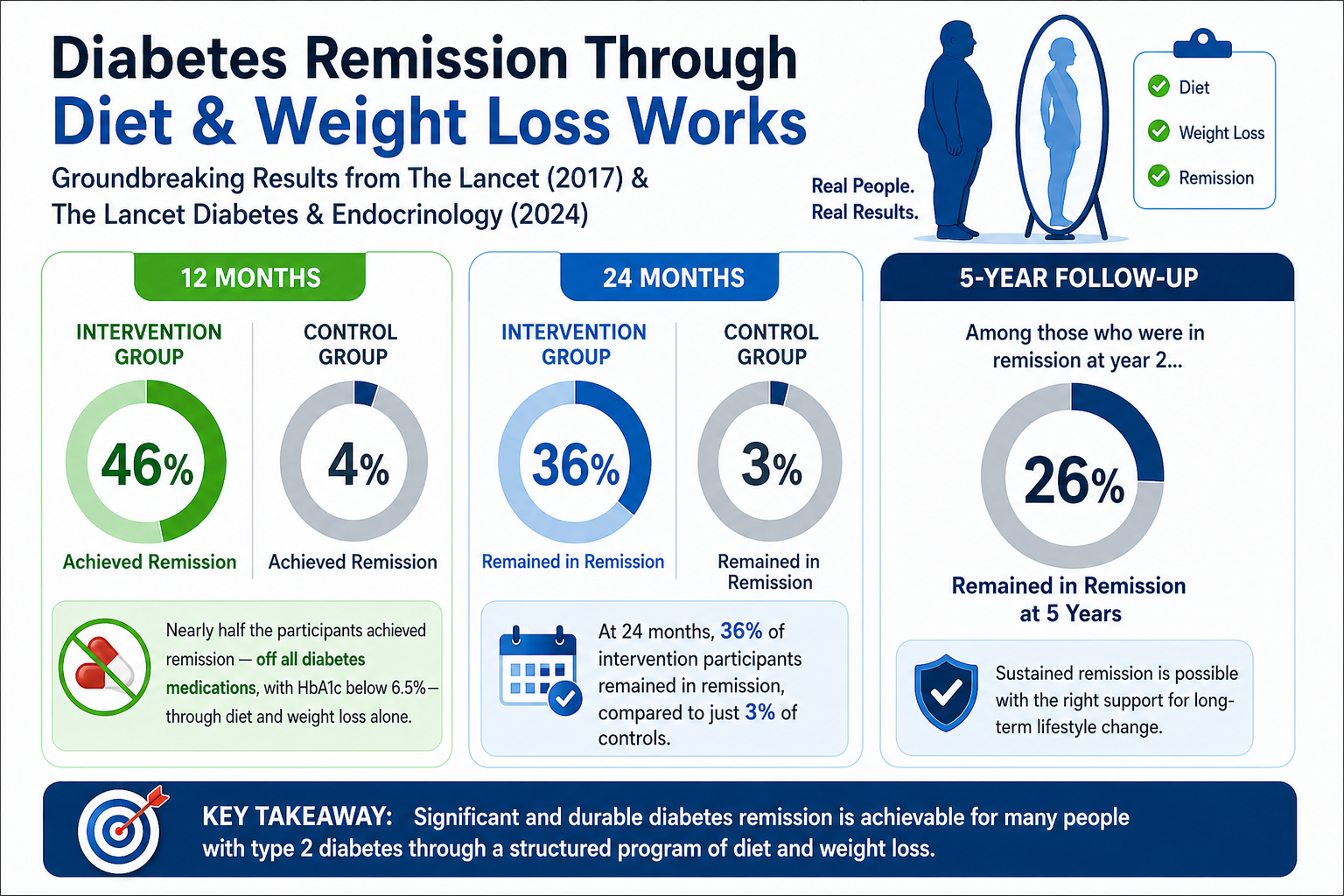
At 12 months, diabetes remission was achieved in 46% of participants in the intervention group, compared to just 4% in the control group. The intervention consisted of withdrawal of antidiabetic and antihypertensive drugs, total diet replacement (825–853 kcal per day formula diet for 12–20 weeks), stepped food reintroduction (2–8 weeks), and then structured support for weight-loss maintenance.
Nearly half the participants achieved remission — off all diabetes medications, with HbA1c below 6.5% — through diet and weight loss alone.
At 24 months, 36% of intervention participants remained in remission, compared to just 3% of controls.
The 5-year follow-up data, published in The Lancet Diabetes & Endocrinology in 2024, showed that of those who were in remission at year 2, 26% remained in remission at 5 years.
Why Does This Matter for You?
Because the DiRECT trial didn’t happen in a specialist research hospital with unlimited resources. It was delivered entirely through primary care — regular doctors and nurses, the same setting most Americans interact with every day.
That’s the point. This wasn’t a proof-of-concept lab experiment. It was a real-world test of whether remission is achievable outside elite medical centres.
The answer was yes.
The Critical Takeaway
The DiRECT trial established one thing above everything else — weight loss is the single most powerful driver of type 2 diabetes remission. The more weight lost, the higher the remission rate. We’ll look at exactly how much in the next section.
Sources: Lean et al. Primary care-led weight management for remission of type 2 diabetes (DiRECT). The Lancet. 2018. 🔗 https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(17)33102-1/abstract
5-Year Extension. The Lancet Diabetes & Endocrinology. 2024. 🔗 https://www.thelancet.com/journals/landia/article/PIIS2213-8587(23)00385-6/fulltext
How much weight loss is needed?
This is probably the question most people want answered first.
“Do I need to lose a little weight — or a lot?”
The honest answer is: the more you lose, the better your chances. But even modest weight loss can make a real difference. Let’s break it down simply.
The Numbers From the DiRECT Trial
The DiRECT trial gave us the clearest picture we’ve ever had of how weight loss and remission are connected. Here’s what the data actually showed:
People who lost more than 15 kg (about 33 lbs) had remission rates of 86% at one year and 82% at two years.
Those who lost more than 10 kg (about 22 lbs) still had remission rates above 75%.
Read those numbers again. That’s not a small effect. That’s the majority of people achieving remission — just through weight loss.
Here’s a simple way to visualise it:
| Weight Lost | Chance of Remission |
|---|---|
| Less than 5 kg (11 lbs) | Very low |
| 5–10 kg (11–22 lbs) | Moderate |
| 10–15 kg (22–33 lbs) | Above 75% |
| More than 15 kg (33+ lbs) | Around 86% |
But Why Does Weight Loss Work?
This is the part most people don’t fully understand — and it’s actually fascinating.
Type 2 diabetes isn’t just about sugar. At its core, it’s heavily linked to excess fat stored in the wrong places — specifically in your liver and pancreas.
When you lose enough weight, fat is removed from the liver and pancreas. This allows your pancreas to start producing insulin properly again — and your liver to stop dumping excess glucose into your bloodstream.
In other words, losing weight doesn’t just improve your blood sugar numbers. It can actually restore the normal function of the organs that manage your blood sugar in the first place.
That’s why remission is possible — and that’s why weight loss is the single most powerful tool available.
What If You Can’t Lose That Much?
Here’s the encouraging part.
You don’t have to hit a specific magic number to see benefits. Any meaningful weight loss moves you in the right direction — improving blood sugar control, reducing medication needs, and lowering your risk of complications.
Remission of short-duration type 2 diabetes will usually require 10–15% of total body weight loss. So for a 200-pound person, that’s roughly 20–30 pounds.
That’s a real, achievable goal — not an unrealistic one.
Source: https://www.frontiersin.org/articles/10.3389/fendo.2022.888557/full
Low-calorie diet approach (800 kcal/day protocol)
If you’ve read about diabetes remission online, you may have come across something called the 800 calorie diet.
It sounds extreme. Maybe even a little scary.
But this is actually the most well-researched dietary approach for type 2 diabetes remission we have — and understanding how it works might surprise you.
What Is the 800 Calorie Protocol?
It’s a structured, short-term diet where your total daily food intake is reduced to around 800 calories per day.
The medical term for this is a Very Low Calorie Diet — or VLCD.
Very low calorie diets typically provide between 400 and 800 calories per day and can result in 20–30% reductions in body weight — sometimes in just 12 to 16 weeks.
In the DiRECT trial, participants followed a slightly more specific version — a total diet replacement programme of 825 to 853 calories per day for 12 to 20 weeks, followed by a structured food reintroduction phase over 2 to 8 weeks.
During the meal replacement phase, people swap their regular meals for specially formulated soups, shakes, and bars that provide controlled calories while still covering essential nutrients.
How Does It Actually Work in Practice?
Here’s a simple breakdown of how the programme typically runs:
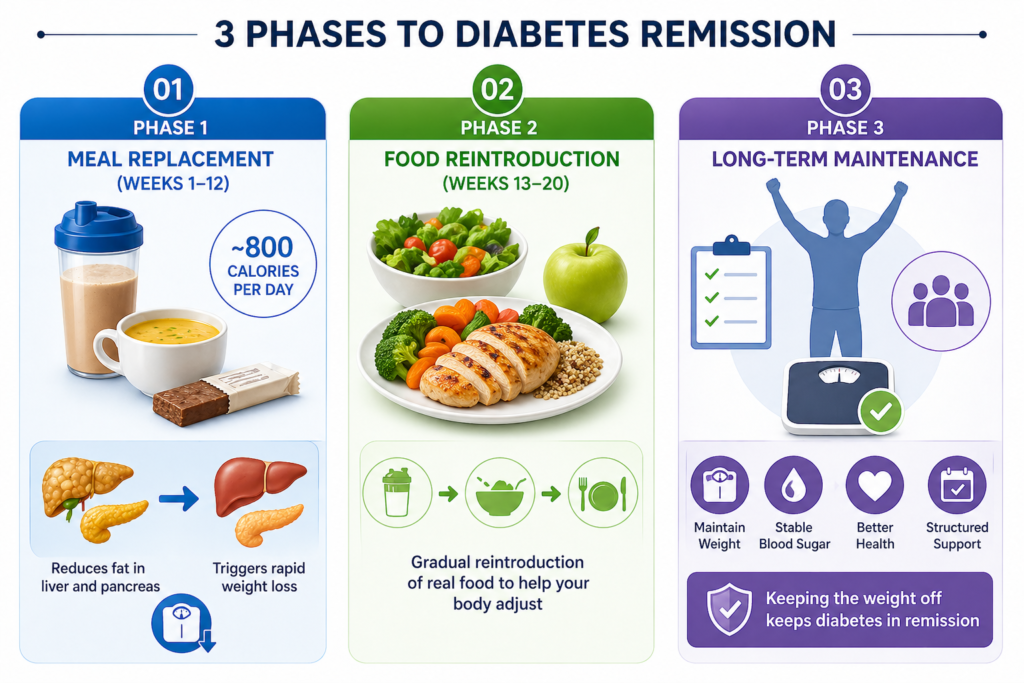
Phase 1 — Meal Replacement (Weeks 1–12) All regular meals are replaced with formula products — shakes, soups, or bars — totalling around 800 calories per day. This phase triggers rapid weight loss and quickly reduces fat in the liver and pancreas.
Phase 2 — Food Reintroduction (Weeks 13–20) Real food is gradually reintroduced — carefully and systematically — to help your body adjust without weight regain.
Phase 3 — Long-Term Maintenance This is the most critical phase. Structured support helps you maintain the weight you’ve lost — because keeping the weight off is what keeps diabetes in remission.
Does It Actually Work?
The evidence says yes — when done properly and with support.
In the DiRECT trial, nearly half the people on an 800 calorie diet achieved remission. Over three quarters successfully stopped their diabetes medication. And nearly 9 out of 10 people who lost more than 15 kg were in remission at one year.
Those are remarkable numbers for a non-surgical intervention.
Is It Safe?
This is the question everyone — understandably — asks first.
A very low calorie diet is not something you should try alone or without medical supervision. This is especially important if you are currently taking diabetes medications or blood pressure drugs, because your medication doses will likely need to be adjusted quickly as your blood sugar improves.
VLCD approaches have shown the most effectiveness in producing rapid weight loss, improving the pancreas’s ability to produce insulin, and reducing HbA1c to pre-diabetic or non-diabetic levels — sometimes within just days.
But done without guidance, the same rapid changes that make it effective can also make it risky.
Always work with your doctor before starting any very low calorie programme.
Source: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8234895/
Low-Carbohydrate Diet and Remission — What the Evidence Says
Not everyone wants to live on meal replacement shakes for three months.
And honestly? That’s completely understandable.
The good news is there’s another well-researched path to remission — one that involves real food, no calorie counting, and a fundamentally different approach to eating.
It’s called a low-carbohydrate diet — and the evidence behind it is growing fast.
What Is a Low-Carbohydrate Diet?
Simply put, it means significantly reducing the amount of carbohydrates you eat each day — things like bread, rice, pasta, sugary drinks, potatoes, and processed snacks.
There are different versions:
- Low-carb — typically under 130 grams of carbs per day
- Very low-carb / ketogenic — under 50 grams per day, sometimes as low as 20–30 grams
The idea behind cutting carbs for diabetes is straightforward. Carbohydrates raise blood sugar. Eat fewer carbs, and your blood sugar spikes less. Over time, this reduces the demand on your pancreas and can improve insulin sensitivity significantly.
What Does the Research Actually Show?
A 2025 systematic review evaluating low-carbohydrate and ketogenic diets in type 2 diabetes found significant reductions in HbA1c, body weight, BMI, and blood pressure. Remission rates were highest at one year — reaching up to 62% — but declined to around 13% by year five.
Those numbers tell an important story. The low-carb approach works — especially in the short to medium term. The challenge, as with most dietary changes, is sticking with it long term.
The Virta Health Study — A Real-World Example
One of the most compelling real-world examples of low-carb diets for diabetes remission comes from Virta Health — a US-based digital health company that paired a very low-carb diet with continuous remote coaching and medical supervision.
Participants followed a very low-carb diet starting at just 30 grams of total carbs per day, with ongoing support from a registered dietitian and a medical care provider.
The five-year results, published in 2024, showed that long-term remission of type 2 diabetes is feasible with a carbohydrate-restricted nutrition approach combined with continuous remote support from an expert care team.
What made Virta different wasn’t just the diet — it was the ongoing coaching and accountability that helped people actually stay on track.
Low-Carb vs. Low-Calorie — Which Is Better?
This is one of the most common questions people ask — and the honest answer is: both work, and neither is clearly superior for everyone.
Research shows that both calorie-restricted and unrestricted low-carbohydrate diets produced meaningful weight loss and HbA1c reductions. Calorie restriction was not shown to be superior to low-carb eating at 12 or 24 months.
What matters most — regardless of the approach — is whether you can sustain it.
Here’s a simple side-by-side comparison:
| Points to consider | Low-Calorie (800 kcal) | Low-Carbohydrate |
|---|---|---|
| Approach | Calorie restriction | Carb restriction |
| Speed of results | Fast | Moderate |
| Requires counting | Calories | Carbs |
| Meal replacements | Often yes | No |
| Sustainability | Harder long-term | More flexible |
| Evidence strength | Very strong (DiRECT) | Strong and growing |
The Bottom Line
A low-carb diet is a legitimate, evidence-backed path to remission — particularly for people who want to eat real food and prefer a more flexible, sustainable approach over a structured meal replacement programme.
The catch? Like any dietary approach, results depend heavily on how consistently you follow it — and how much support you have along the way.
In the next section, we look at the most dramatic intervention of all — one that produces the highest remission rates of anything we’ve discussed so far.
Sources: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12476234/, https://www.diabetesresearchclinicalpractice.com/article/S0168-8227(24)00808-8/fulltext
6. Bariatric Surgery — The Most Powerful Remission Tool We Have
When it comes to producing the highest remission rates of any intervention available, bariatric surgery stands in a league of its own.
It’s not for everyone. But the data is hard to ignore.
What Is It?
Bariatric surgery — also called weight-loss or metabolic surgery — changes how your digestive system works to produce significant, lasting weight loss. The two most effective types for diabetes remission are gastric bypass and sleeve gastrectomy.
What Does the Research Show?
A major NIH-funded study published in JAMA in 2024 followed patients for up to 12 years. People with type 2 diabetes who underwent bariatric surgery achieved better long-term blood glucose control than those who received medical management plus lifestyle interventions — and had higher rates of diabetes remission up to 12 years post-surgery.
The financial case is compelling too. At three years, people who had bariatric surgery had 56% higher remission rates than those who didn’t — and healthcare costs were over $20,000 lower in the years following the procedure.
Why Does It Work So Well?
Surgery doesn’t just work because you eat less. Gastric bypass in particular triggers rapid hormonal changes that improve blood sugar — sometimes within days of surgery, before major weight loss has even occurred. That’s why doctors now call it metabolic surgery.
Who Qualifies?
In the US, surgery is generally considered for people with:
- BMI of 35 or higher with type 2 diabetes
- BMI of 30–34.9 with poorly controlled diabetes
The ADA formally recognises bariatric surgery as a legitimate treatment option for type 2 diabetes.
7. Who Is Most Likely to Achieve Remission?
Remission is possible for many people — but it’s more likely for some than others. Here’s what the research tells us.
A large Kaiser Permanente study published in Diabetes Care reviewed over 550,000 adults with type 2 diabetes. The findings were clear:
Younger adults had higher odds of remission compared to older adults. People diagnosed less than a year earlier were significantly more likely to achieve remission than those who had been living with diabetes for four or more years. Adults with a baseline HbA1c below 7% were more likely to go into remission — and those taking multiple glucose-lowering drugs were significantly less likely to achieve remission than those on fewer medications
The DiRECT trial data tells the same story. Remission is a realistic aspiration for most people with type 2 diabetes diagnosed within six years — and achieving at least 10 kg of weight loss should be a primary target.
In simple terms, your best chances look like this:
| Factor | Better Odds of Remission |
|---|---|
| Time since diagnosis | Less than 6 years |
| HbA1c at start | Below 7% |
| Medications | Fewer glucose-lowering drugs |
| Weight loss achieved | 10 kg (22 lbs) or more |
| Age | Younger adults |
But Here’s the Most Important Thing
None of these factors rules you out completely.
Patients with shorter disease duration, lower baseline HbA1c, greater weight loss, no prior insulin therapy, and fewer medications were more likely to achieve remission — but weight loss remains the strongest single predictor across all groups.
In other words — the single most powerful thing you can do, regardless of where you start, is work toward meaningful weight loss with proper medical support.
Source: https://divisionofresearch.kaiserpermanente.org/type-2-diabetes-remission/
https://onlinelibrary.wiley.com/doi/10.1111/dme.14395
FAQ
Q.1 Can type 2 diabetes go away permanently?
Type 2 diabetes cannot be fully cured — but it can go into remission.
Remission means blood sugar returns to normal without medication. This is possible through:
Significant weight loss of 10–15 kg
Bariatric surgery
Strict low calorie diet
Consistent exercise and lifestyle changes.
Q.2 What’s the quickest way to reverse type 2 diabetes?
The fastest evidence-based method is a very low calorie diet (800 kcal/day) combined with significant weight loss — proven by the landmark DiRECT Trial.
This works best in:
Newly diagnosed patients
Those diagnosed less than 6 years ago
Significantly overweight patients
Remember — no supplement or magic drink reverses diabetes. Consistent weight loss through diet and exercise is the only proven method.
Q.3 How Long Does It Take to Reverse Type 2 Diabetes?
Reversal typically takes 3–6 months of consistent lifestyle changes. The landmark DiRECT Trial showed remission in 8–12 weeks with an 800 kcal/day diet.
Results depend on:
How long you’ve had diabetes.
How much weight you lose.
How strictly you follow diet and exercise.
Q.4 Can Type 2 Diabetes Be Reversed Without Medication?
Yes — in early stages, Type 2 diabetes can go into remission without medication through:
Significant weight loss
Low calorie diet
Regular exercise
However this is more likely in newly diagnosed patients. Long-term diabetics may still need medication alongside lifestyle changes.
Q.5 Can We Reverse Type 2 Diabetes in 3 Months?
Yes — research shows remission is possible within 3 months through an intensive 800 kcal/day very low calorie diet and significant weight loss.
However results vary based on:
Duration of diabetes
Amount of weight lost
Consistency of lifestyle changes
Not everyone achieves remission in 3 months — but meaningful improvement is almost always seen.
Reference
1. Remission Definition — ADA Consensus Report Riddle MC et al. Diabetes Care. 2021. 🔗 https://diabetesjournals.org/care/article/44/10/2438/138556
2. DiRECT Trial — Primary & Long-Term Results Lean MEJ et al. The Lancet. 2018 + 5-Year Extension. 2024. 🔗 https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(17)33102-1/abstract
3. Weight Loss & Remission Rates — DiRECT Data Lean MEJ et al. Frontiers in Endocrinology. 2022. 🔗 https://www.frontiersin.org/articles/10.3389/fendo.2022.888557/full
4. Very Low-Calorie Diet & T2D Remission — Narrative Review Juray S et al. Nutrients. 2021. 🔗 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8234895/
5. Low-Carbohydrate Diet Long-Term Efficacy — Systematic Review Das R et al. Cureus. 2025. 🔗 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12476234/
6. Bariatric Surgery vs Medical Management — 12-Year Outcomes Courcoulas AP et al. JAMA. 2024. 🔗 https://www.nih.gov/news-events/news-releases/bariatric-surgery-provides-long-term-blood-glucose-control-type-2-diabetes-remission
7. Predictors of T2D Remission — Kaiser Permanente Study Rodriguez LA et al. Diabetes Care. 2023. 🔗 https://divisionofresearch.kaiserpermanente.org/type-2-diabetes-remission/
About the author
It’s me Mohammad Junaid Rain an MBBS student at GMC Nagpur, passionate about making evidence-based medical information accessible to every Indian. “medstuffs.com” is dedicated to clear, doctor-written disease education for patients and caregivers.
Disclaimer: This article is for educational purposes only and does not substitute professional medical advice. Please consult your doctor for diagnosis and treatment.